

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Effective Pharmacological Treatment Options for Anxiety Disorders
Cumulative research with animal, normative, and clinical populations over several decades shows that the mechanisms underlying anxiety disorders differ from those of the normal emotion of anxiety. In persons with anxiety disorders, fear and tension are disproportionate to the actual threat and may be present when no real threat exists, thereby generating an expectation of danger and distorted perceptions related to danger and various types of threats. The most common anxiety disorders are social anxiety disorder (SAD), generalized anxiety disorder (GAD), and posttraumatic stress disorder (PTSD). Persons with SAD can experience a wide range of social fears as well as severe functional consequences, whereas persons with GAD tend to experience emotional, interpersonal, and somatic symptoms of high levels of chronic anxiety. Persons with PTSD have vivid memories of and thoughts about a terrifying event or ordeal that lead to the development of anxiety, depression, and functional impairment. Effective treatment options-pharmacotherapy; psychotherapy, particularly cognitive-behavioral therapy; or a combination-can be discussed openly with the patient to make a collaborative, informed decision. A variety of medications can be used to successfully manage anxiety disorders, of which SSRIs and serotonin-norepinephrine reuptake inhibitors are the most effective. When properly used, medications can enhance a patient's own efforts to master anxiety; overcome fearful avoidance; and address troubling behaviors, patterns, or memories. (Drug Benefit Trends. 2008;20:101-113)
Cumulative research with animal, normative, and clinical populations over several decades shows that the mechanisms underlying anxiety disorders differ from those of the normal emotion of anxiety. In persons with anxiety disorders, fear and tension are disproportionate to the actual threat and may be present when no real threat exists, thereby generating an expectation of danger and distorted perceptions related to danger and various types of threats. The most common anxiety disorders are social anxiety disorder (SAD), generalized anxiety disorder (GAD), and posttraumatic stress disorder (PTSD). Persons with SAD can experience a wide range of social fears as well as severe functional consequences, whereas persons with GAD tend to experience emotional, interpersonal, and somatic symptoms of high levels of chronic anxiety. Persons with PTSD have vivid memories of and thoughts about a terrifying event or ordeal that lead to the development of anxiety, depression, and functional impairment. Effective treatment options-pharmacotherapy; psychotherapy, particularly cognitive-behavioral therapy; or a combination-can be discussed openly with the patient to make a collaborative, informed decision. A variety of medications can be used to successfully manage anxiety disorders, of which SSRIs and serotonin-norepinephrine reuptake inhibitors are the most effective. When properly used, medications can enhance a patient’s own efforts to master anxiety; overcome fearful avoidance; and address troubling behaviors, patterns, or memories. (Drug Benefit Trends. 2008;20:101-113)
Anxiety disorders are among the most common behavioral health disorders, affecting thousands of persons of all ages and cultural backgrounds (Figure 1).1,2 Because the word "anxiety" now has meanings in both technical and general usage, it is often mistakenly assumed that anxiety disorders are merely extremes of normal emotions rather than conditions with qualitatively distinct syndromes, symptoms, and behaviors. Most emotion theories present "normal" anxiety as an emotion with a complex, multiple-system physiological cascade of activation that occurs in response to a realistic potential threat and prepares a person to act. Pathological anxieties, unlike normal anxiety, are syndromal states of fear, tension, and threat-related perceptions that have no apparent adaptive function, are associated with significant functional impairment, and usually appear disproportionate to the situation to both the clinician and the patient.


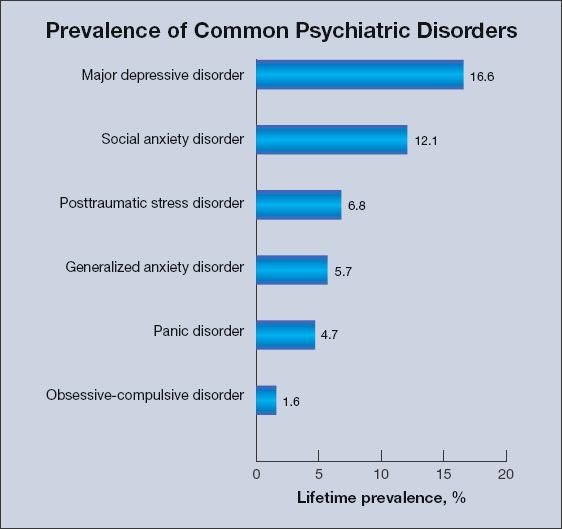
Figure 1. Social anxiety disorder was the most common anxiety disorder among Americans between February 2001 and April 2003. Source: Kessler RC et al.
Arch Gen Psychiatry.
2005.1
Early nosological psychoanalytic models assumed that all anxiety disorders-as well as depressive and psychotic disorders-were extreme forms of normal anxiety (neuroses) and indicated defensive manifestations of marked conflict. For example, persons with social anxiety disorder (SAD) were considered to have an extreme form of shyness because of conflicted assertiveness, while those with obsessive-compulsive disorder were regarded as paralyzed by obsessional conflicts of a sexual and aggressive nature.
As the scientific basis for understanding anxiety becomes more sophisticated, clinical practice can increasingly be based on an emerging, stabilizing foundation of synthetic concepts drawn from multidisciplinary work on neural networks, dynamic psychological drives, abnormal or dysregulated neural pathways, and behavioral outcomes and can move away from simplistic etiological models. For clinicians, there is persuasive proof that severe, functionally paralyzing anxiety disorders respond dramatically to pharmacotherapy as well as to effectively implemented cognitive-behavioral, interpersonal, and supportive-expressive psychotherapies.
A clinician’s confidence in the efficacy of antianxiety medications is usually a powerful means to forming a close alliance with persons who have an anxiety disorder. Once clinicians gain experience and see quantifiable results, it becomes relatively easy to communicate an optimistic understanding of a patient’s emotional condition and to identify ways to relieve the anxiety, often with dramatic improvement in the patient’s overall quality of life.
Contemporary clinical practice is based on the sophisticated skills of recognizing, diagnosing, and treating anxiety disorders. This article focuses on the 3 most common anxiety disorders: SAD, generalized anxiety disorder (GAD), and posttraumatic stress disorder (PTSD). For each disorder, there is considerable scientific literature that recommends various specialized adaptations of cognitive-behavioral therapy (CBT) principles as effective treatments, but this review focuses on the pharmacological literature.
Social Anxiety Disorder
Typically, in persons with generalized SAD, onset of symptomatic impairment occurs in their early teenage years as increasingly complex social interactions evoke severe anxiety, expectations of failure and embarrassment, and behavioral avoidance as a coping strategy.3 Behavioral inhibition, the temperament described by Kagan and colleagues4 as a generally slow, cautious, and avoidant pattern of approach to unfamiliar persons and events, is much more common in early childhood. The average time lag between onset of SAD and a person’s first contact with a behavioral health professional, if treatment is sought at all, is 10 years.1,5 In the United States today, most persons with SAD-like persons with most other behavioral health disorders-do not receive treatment.
Characteristics. Persons with the generalized form of SAD tend to be lonely underachievers. They often do not have a partner; alternatively, they may be in a romantic relationship but have few friends. They experience painful daily struggles when interacting with others in the workplace or school or even when going about such mundane activities as shopping. Persons who have SAD are twice as likely to be on welfare or disability as persons without the disorder.5
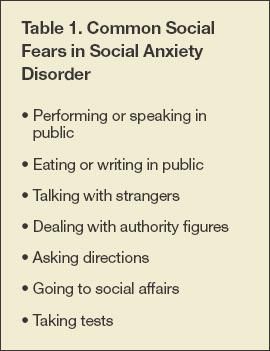
As with all anxiety disorders, exposure to specific activating situations (Table 1) invariably produces symptoms of intense anxiety, even panic, with severe physiological activation, such as sweating, intestinal cramping, or need for frequent urination. Since avoidance temporarily reduces anxiety, it is reinforced over many years. This operant conditioning usually leads to additional problems with school or work achievement, limited functioning in the world, comorbidity with major depressive disorder (MDD), and substance abuse (self-medication). For example, students with severe SAD may exhibit a pattern of feigning illness to avoid exams and may not graduate from high school, college, or graduate school.


Persons with SAD may be able to work but may gravitate toward careers that allow them to work in isolation; others may shun promotions at work because they usually involve increased visibility and leadership duties. Some persons with SAD may have an empty personal life dominated by expectations of rejection and negative evaluation. Clearly, SAD significantly affects a person’s choices and path in life.
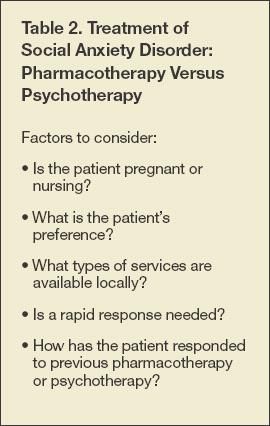
Treatment. When discussing treatment options with patients, clinicians should consider several factors: pharmacotherapy; psychotherapy; or pharmacotherapy combined with psychotherapy, either simultaneously or sequenced (Table 2). With respect to providing evidence-based psychotherapy, it is often difficult for practitioners to find training for themselves or to locate a clinician who specializes in CBT outside major US cities to whom to refer a patient. Educating patients about this option is necessary but can become awkward if the treatment is not easily obtainable. Although rigorous controlled trials have demonstrated the efficacy of CBT over the past 2 decades, most practitioners do not have specialized training because such training is expensive, programs are difficult to find, and older clinicians typically were not initially trained in the basic principles and skill sets of CBT.6 On the other hand, there may be reasons to avoid prescribing medications (eg, the patient is pregnant or nursing; drug-drug interaction concerns) or a patient may have strong preferences regarding treatment, in which case psychosocial treatment should be provided or sought for the patient.


The SAD literature demonstrates 2 overall patterns: (1) medication and CBT appear equally effective; and (2) medication tends to work somewhat faster than CBT, but CBT produces more significant results, with lower rates of relapse.7,8 If a patient has paralyzing symptoms, has severe depression, or prefers medication, typically he or she is initially given medication, which is sometimes combined with evidence-based psychotherapy; for other patients, psychotherapy treatment is considered after the clinician evaluates the patient’s response to the pharmacotherapy.
The clinician should also ask patients how often fearful situations arise during the course of their daily life. For example, a patient who is afraid of delivering an annual report at work might be so anxious that he starts losing sleep 6 weeks before the speech date. He might lose weight because he is too anxious to eat but otherwise is fine. This patient would not be a candidate for a yearlong course of daily medication given the time-limited nature of his particular stress-diathesis profile. Instead, using either evidence-based time-limited therapy or a medication for only a few weeks to treat this patient would be most prudent.
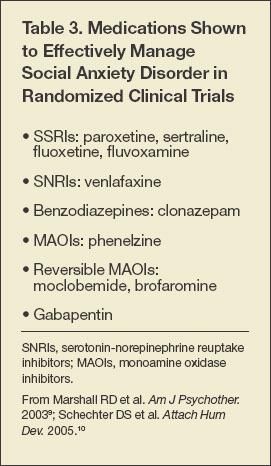
There are a number of clinical trials, including large multiple-site trials, testing the efficacy of various medications for reducing SAD symptoms (Table 3).9,10 However, few trials compare one drug with another. Meta-analytic methods suggest several conclusions: (1) the most compelling overall evidence supports the use of SSRIs and monoamine oxidase inhibitors (MAOIs); (2) there is significant variation across the different classes of medications; and (3) within each class, the degree of clinical response appears similar when there are replicated, randomized clinical trials. Clonazepam, a benzodiazepine, was found to be highly effective in 1 trial.11 Other medications used for the treatment of persons with SAD include gabapentin, which was found to be modestly effective, and brofaromine, a reversible MAOI not available in the United States. β-Blockers continue to be widely used, particularly for persons with performance anxiety, despite the lack of demonstrated efficacy in this subgroup.


Relatively few studies examine either long-term treatment for persons with SAD or optimal length of treatment. However, there is solid clinical evidence of the long-term (up to 1 year) efficacy of the SSRI sertraline (Figure 2).9,12,13 There is no reason to suspect the findings will be any different for other related medications prescribed to treat persons with SAD. In general, practitioners can expect to achieve about a 50% improvement in response to medication, but there is significant individual variation in treatment response.9,11


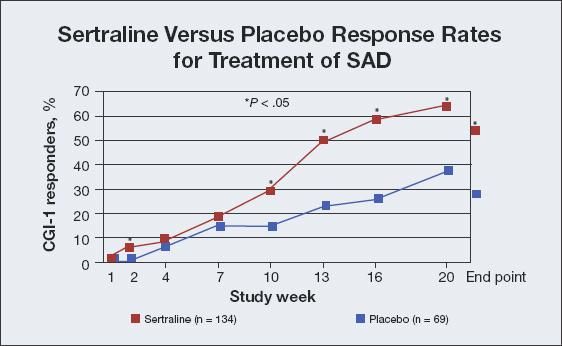
Figure 2. In Clinical Global Impressions responders who were very much improved (CGI-1 responders), sertraline reduced symptoms of social anxiety disorder (SAD) by an approximate 50% improvement in symptoms compared with an approximate 30% response achieved with placebo at the end of treatment. Sources: CGI; Van Ameringen MA et al.
Am J Psychiatry.
2001.12
When used to treat persons with SAD, SSRIs and MAOIs are dosed the same as they are for treating those with depression. While there is some evidence from uncontrolled studies to indicate that a higher dosage might be more effective, taking a conservative approach to dosing enables a clinician to assess whether a patient is responding to a lower dosage-which can improve patient adherence to the medication regimen because lower dosages carry less risk of adverse effects.
Strategies of augmentation involve adding a second medication to a drug regimen that has produced partial or no improvement, with minimal or no adverse effects for the patient. Examples include adding buspirone to an SSRI14 and clonazepam to an SSRI or serotonin-norepinephrine reuptake inhibitor (SNRI) if there are no contraindications to using a benzodiazepine. (Anecdotal evidence suggests that the latter combination can produce good outcomes and should be studied further.) Many clinicians reserve prescribing the MAOI phenelzine, which has been shown to be effective in several clinical trials, for persons with SAD who do not want to enter CBT or who respond suboptimally to an SSRI. Taking phenelzine requires that the patient adhere to a special diet to avoid potentially dangerous food-drug interactions.
Practitioners should be cautious about prescribing an atypical antipsychotic medication for a person with SAD. Adverse effects can lead to cognitive impairment. In general, after clinicians have assessed and tried the major classes of medications for a particular patient, they should consider CBT, which clinical guidelines suggest is more likely to be effective than combination therapy.
Generalized Anxiety Disorder
The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), defines GAD as excessive, uncontrollable, physically manifested anxiety and worry.2
Characteristics. GAD is characterized by the following2:
• Worry is present across a number of domains.
• Worry is present on most days for the past 6 months.Worry is difficult to control.
In addition, the DSM-IV specifies that for anxiety to be categorized as GAD, the person must have at least 3 of 6 associated symptoms:
• Emotional/cognitive: irritability or difficulty in concentrating.
• Physical: restlessness, easy fatigue, muscle tension, sleep disturbance.
A person with GAD must exhibit a behavior pattern that is often self-described as “being a worrier”; that is, worry is not limited to 1 or 2 specific concerns but is present in several areas and tends to dominate the person’s approach to life. Persons with GAD immediately answer “yes” to the question “Are you a worrier?” They find things to worry about, such as losing their home or job, suffering during a weather emergency, or having their children become seriously ill or involved in a motor vehicle accident. Through psychotherapy, persons who have GAD may realize that they are motivated by the unconscious belief that worrying-being “ever vigilant”- will somehow protect them from catastrophe.
Judging the symptoms of a person with GAD to be “excessive” and “unreasonable” remains a subject of debate, since what is normative in a group is influenced by class, culture, personality traits, values, temperament, and life experiences. A person’s level of worry can often be understandable in the context of his life while simultaneously being maladaptive. For example, a person who grew up during the Great Depression may demonstrate unnecessary worry about money, health, and family. Treating such a person, whose symptoms are readily understandable, can improve the overall quality of his life. If GAD develops in a person after a series of traumatic life events, he may benefit from pharmacotherapy once other common disorders, such as PTSD or MDD, have been eliminated in the differential diagnosis.
Comorbidity is high (60% to 90%), particularly with MDD.15,16 In most persons, onset of GAD precedes that of MDD, just as it does in persons with SAD.17
The worry associated with GAD is usually accompanied by physical symptoms, particularly fatigue, headaches, muscle tension, muscle aches, and other symptoms of increased chronic anxiety. As a result, persons with GAD often present several times to an internist, who, ideally, recognizes a mental health issue and either refers these patients to a psychiatrist or other behavioral health professional or attempts to help them using an evidence-based treatment.
Treatment. Persons who have GAD often respond best to a combination of pharmacotherapy and psychotherapy; this is currently the general recommendation for achieving long-term benefits. Evidence-based psychotherapies adapt the CBT model to raise patients’ awareness of their self-perpetuating fears and worries, as well as to assist them in articulating, confronting, questioning, and overcoming their assumptions and expectations of catastrophes.
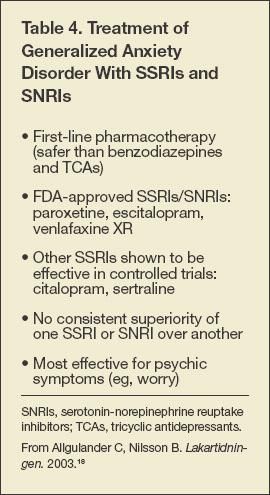
SSRIs and SNRIs. These are the first-line therapies used to control the symptoms of persons with GAD because of their acute and long-term effectiveness and relative safety compared with other treatment options (Table 4).18 The symptoms that appear to be best controlled with medication are cognitive worry, rumination, and obsession with catastrophe. Paroxetine, escitalopram, venlafaxine, citalopram, and sertraline have been found to be similarly effective in clinical trials.19 Gelenberg and colleagues20 found venlafaxine to be superior to placebo during a 6-month randomized controlled trial. Similar to results of studies of persons with SAD, active treatment produces approximately a 50% improvement in symptoms, compared with a 30% improvement observed with placebo. The same is true of escitalopram studies, which show improvements in symptoms averaging 50% and 25% to 30% in active treatment and placebo groups, respectively.21


The remission rate in these medication trials is consistently low: only 10% to 30% of patients are considered to be free of symptoms and functional impairment following treatment. This finding confirms the value of combining pharmacotherapy with CBT whenever possible; even brief psychotherapy sessions improve patient outcomes.
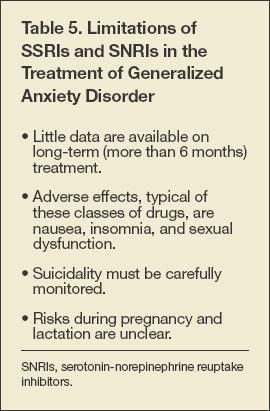
Another limitation in the GAD literature is the lack of long-term (more than 6 months) data on patient outcomes associated with the use of SSRIs and SNRIs. Most researchers recommend continuing to give patients medication for at least 1 year and slowly tapering off the medication only after several months of stable symptom improvement. Patients often fear a relapse-in other words, they are worriers about this as well-and the use of CBT techniques may be particularly effective in this situation if tapering off the medication is advisable. Ultimately, once informed about their choices, patients will need to make treatment decisions themselves. Other limitations of treating persons with GAD using SSRIs and SNRIs are listed in Table 5.


Benzodiazepines. Concerns about dependence and withdrawal symptoms-especially seizure-have led to clonazepam, lorazepam, and diazepam to be considered as second-line agents for persons with GAD. Patients must be informed of the dangers of forgetting to take or otherwise abruptly discontinuing their medication.
The efficacy of benzodiazepines, however, is similar to that of SSRIs.22-26 Benzodiazepines tend to be more effective for controlling hyperarousal, or physiological symptoms of anxiety, whereas SSRIs may be better for managing cognitive and psychological symptoms.
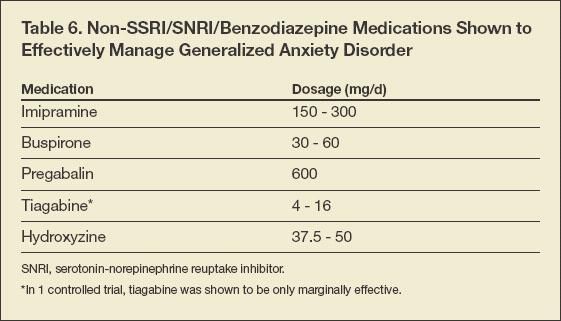
Other medications that can be used to treat persons with GAD are listed in Table 6. As with all anxiety disorders, a psychiatrist might need to periodically revisit and revise a patient’s treatment plan based on his response to medications and changing preferences.


Posttraumatic Stress Disorder
In adults, PTSD can develop after a traumatic event, specifically defined as experiencing or witnessing threatened death or injury to themselves or others. In children who are sexually abused, PTSD can develop in the absence of this threat when sexual abuse occurs in the context of a pedophilic seduction rather than violent threats or overt coercion.
Characteristics. The subjective response to trauma in PTSD must be intense and in the negative affective range. Reactions include fear, helplessness, horror, dissociation, rage, and sudden numbness.27 A powerful emotional response to the traumatic event itself is predictive of subsequent PTSD.11
Persons are given a diagnosis of PTSD based on the following symptoms2:
• Reliving the triggering event in the form of thoughts, dreams, or vivid images. Persons with PTSD rarely have true flashbacks, which are vivid, visual reenactments that occur when they are in a dissociative state. While reliving the event, they lose some contact with reality.
• Avoiding reminders of the trauma.
• Experiencing numbing of positive emotion. Patients, especially those with depression, often describe feeling dead inside; they have no feelings of joy or tenderness, and typically have lost interest in sex. Positive emotions are scarce, whereas negative feelings of anger, resentment, depression, fear, and anxiety are common.
Most persons who experience trauma eventually recover.11 This does not mean that the trauma was not powerful or life-changing. In many cases, a person arrives at a balance between positive and negative feelings about the experience. For example, while studying Vietnam veterans, Dohrenwend and colleagues28 found that most of the veterans reported having positive or mixed feelings about their experience (eg, those reporting positive feelings indicated that their experience had taught them values and priorities as well as led to personal growth). The researchers also found that these veterans were the most functional.
Evidence suggests that PTSD occurs on a continuum.29,30 Persons can experience the symptoms of PTSD as specified in the DSM-IV, but at a level that falls below the diagnostic criteria-for example, they might have 1 reexperiencing symptom, 2 avoidance symptoms, and 1 hyperarousal symptom. However, several studies have shown that subthreshold PTSD is also associated with impairment. Research involving survivors of the 9/11 attacks showed that there are 4 times as many persons with subthreshold PTSD as there are with full PTSD.31 Furthermore, rates of suicidal ideation increase with the number of PTSD symptoms.29
Treatment. Many treatment options are available for persons with PTSD. The patient and clinician can choose among psychotherapy, pharmacotherapy, or a combination of both.
The primary types of psychotherapy used to treat persons with PTSD are exposure therapy, cognitive therapy, stress inoculation training, and eye movement desensitization and reprocessing. Pharmacotherapy includes SSRIs, MAOIs, mood stabilizers, antianxiety agents, and antipsychotic medications.32 Tricyclic antidepressants (TCAs) have been shown to be modestly effective for managing PTSD; however, TCAs have not been studied as extensively as SSRIs. Clinical guidelines recommend starting with monotherapy, progressing through trials of various medications if the patient is initially unresponsive (Figure 3). Patients who are partial responders to an SSRI or venlafaxine might respond to the addition of a mood stabilizer (valproate, lamotrigine, topiramate, carbamazepine, lithium) or an atypical antipsychotic (olanzapine, risperidone, quetiapine) to the regimen (Figure 4).

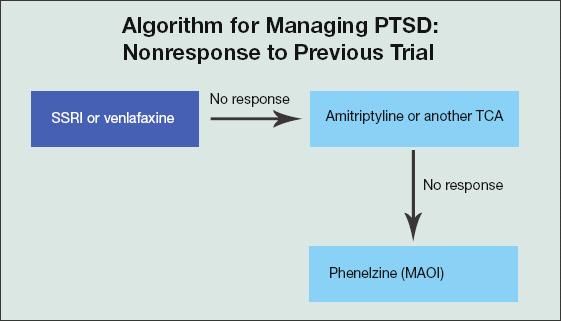
Figure 3. Evidence-based treatment of posttraumatic stress disorder (PTSD) begins with an SSRI or venlafaxine. If the patient does not respond, this medication is discontinued and the patient begins a trial of amitriptyline or another tricyclic antidepressant (TCA). If this fails to adequately control symptoms, changing to a monoamine oxidase inhibitor (MAOI), such as phenelzine, might improve the patient’s outcome.


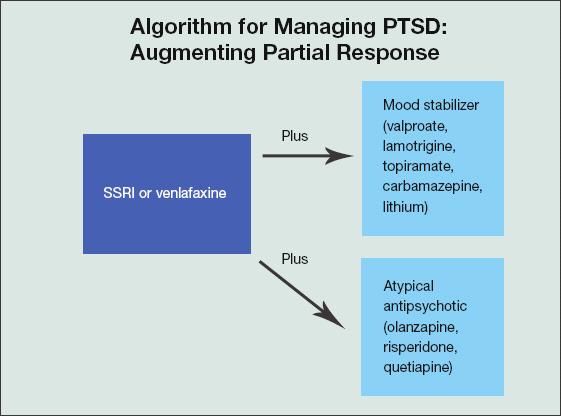
Figure 4. A person with posttraumatic stress disorder (PTSD) who responds only partially to an SSRI or venlafaxine may respond to the addition of a mood stabilizer (valproate, lamotrigine, topiramate, carbamazepine, lithium) or an atypical antipsychotic (olanzapine, risperidone, quetiapine) to his or her evidence-based medication regimen.
As with other anxiety disorders, using medication to treat persons with PTSD averages a 50% to 60% improvement in symptoms for active treatment, compared with an approximate 30% improvement for persons taking placebo.32 For example, in a comparison of 2 dosages of paroxetine, 20 mg/d or 40 mg/d, with a placebo in a multiple-site trial of 551 persons with PTSD, the percentage of responders averaged 63% for paroxetine 20 mg/d; 57% for paroxetine 40 mg/d (the difference in response rates to the 2 dosages of paroxetine was statistically insignificant); and 37% for placebo.33 Men and women responded equally well to treatment with both dosages of paroxetine. Other trials comparing placebo with active treatment with fluoxetine34 and sertraline11 showed similar response rates.
More recently, Davidson and colleagues35 compared remission rates in persons with PTSD who were treated with venlafaxine XR, sertraline, or placebo. Remission rates at 12 weeks averaged 30.2% for the venlafaxine XR group, 24.3% for the sertraline group, and 19.6% for the placebo group. Thus, most persons with PTSD can expect to have some symptoms even after treatment with a medication.
Few studies have examined the effects of long-term treatment on persons with PTSD. In one study, Londborg and colleagues36 continued treatment with sertraline for 36 weeks. The most rapid response occurred during the first 12 weeks of treatment; however, patients continued to improve until the study end point. Medications help patients in part by restoring their capacity to process the trauma so they can move forward with their lives, which can take months. Research shows that stopping treatment too early (within 6 months) can lead to relapse or clinical deterioration; for this reason, patients are advised to continue treatment for at least 1 year.
Mood stabilizers and atypical antipsychotics act as adjuncts to the SSRI or venlafaxine. There is little evidence indicating that they are effective or appropriate as monotherapy. One study of olanzapine monotherapy showed it to be no more effective than placebo.6
Negative trials. Some trials involving persons with PTSD and other anxiety disorders show that treatment is no better than placebo or produces negative results. Some of these were small studies, some were unpublished, and some involved populations at Veterans Administration hospitals and Vietnam veterans. The implications of these studies are unclear.
A note of caution concerns the use of benzodiazepines. Two studies reported poor outcomes in persons who received benzodiazepines in the acute aftermath of trauma. One study showed that 69% of persons with acute PTSD who were given a benzodiazepine had PTSD at follow-up versus only 15% of those given placebo.37 In the other study, 55% of patients taking benzodiazepines had PTSD at follow-up versus 27% of those given placebo.38 The patients given high-dose benzodiazepines were 2 to 4 times more likely than those given placebo to progress from acute to chronic PTSD.
Conclusion
Treatment of patients with anxiety disorders can be challenging for a number of reasons, but the primary barrier to patients receiving evidence-based treatment to date is that they do not receive the correct diagnosis. Once the diagnosis is clearly determined, the clinician can share this information with patients and in this way communicate both optimism and expertise. A discussion of treatment options generally needs to allow for addressing patients’ anxieties about their treatment. This article provides a review of the medications available for persons with anxiety disorders as well as some guidelines and clinical recommendations that will make the process of providing effective treatment more successful for both the physician and the patient.
ADDRESSING COMMON MISCONCEPTIONS ABOUT TREATING ANXIETY DISORDERS
When exploring treatment options with patients, clinicians should dispel some common misconceptions about treatment while stressing positive messages and strategies. A patient’s objections to taking medication may reflect cognitive distortions that can be addressed in psychotherapy. Common distortions include the following:
• Medication is a sign of personal failure or an inability to cope.
• Needing medication means that psychotherapy has failed.
• Medication is evidence of the clinician’s lack of personal interest.
• Medication numbs or suppresses normal emotions.
• Taking medication prevents dealing with the “real” problem.
• Medication erases past trauma.
• Medication provides a magical rescue from complex problems.
When discussing the use of medications with patients, clinicians should focus on the following positive concepts:
• Identify medication as an aid to personal efforts to deal with stress and trauma.
• Reassure patients that revisiting and processing the trauma is the body’s way of healing and that medications can help.
• Identify catastrophic thinking (ie, expecting the worst in every situation), illustrate the way past trauma has influenced this way of viewing the world and the future, and suggest a more helpful alternative framework to use in approaching treatment.
• Encourage deliberate and systematic reversal of avoidance behavioral patterns.
• Offer praise and support for patients’ efforts to embrace healing.
References:
References
- 1. Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:593-602.
- 2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Washington, DC: American Psychiatric Press; 1994.
- 3. Rapee RM, Spence SH. The etiology of social phobia: empirical evidence and an initial model. Clin Psychol Rev. 2004;24:737-767.
- 4. Kagan J, Reznick JS, Snidman N. The physiology and psychology of behavioral inhibition in children. Child Dev. 1987;58:1459-1473.
- 5. Schneier FR, Johnson J, Hornig CD, et al. Social phobia. Comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. 1992;49:282-288.
- 6. Davidson JR. Pharmacotherapy of social anxiety disorder: what does the evidence tell us? J Clin Psychiatry. 2006;67(suppl 12):20-26.
- 7. Walker KL, Chestnut D. The role of ethnocultural variables in response to terrorism. Cultur Divers Ethnic Minor Psychol. 2003;9:251-262.
- 8. Marshall RD, Spitzer R, Liebowitz MR. Review and critique of the new DSM-IV diagnosis of acute stress disorder. Am J Psychiatry. 1999;156:1677-1685.
- 9. Marshall RD, Carcamo JH, Blanco C, Liebowitz M. Trauma-focused psychotherapy after a trial of medication for chronic PTSD: pilot observations. Am J Psychother. 2003;57:374-383.
- 10. Schechter DS, Coots T, Zeanah CH, et al. Maternal mental representations of the child in an inner-city clinical sample: violence-related posttraumatic stress and reflective functioning. Attach Hum Dev. 2005;7:313-331.
- 11. Ballenger JC, Davidson JR, Lecrubier Y, et al. Consensus statement update on posttraumatic stress disorder from the international consensus group on depression and anxiety. J Clin Psychiatry. 2004;65(suppl 1):55-62.
- 12. Van Ameringen MA, Lane RM, Walker JR, et al. Sertraline treatment of generalized social phobia: a 20-week, double-blind, placebo-controlled study. Am J Psychiatry. 2001;158:275-281.
- 13. Rich S, Rubin L, Walker AM, et al. Anorexigens and pulmonary hypertension in the United States: results from the surveillance of North American pulmonary hypertension. Chest. 2000;117:870-874.
- 14. Van Ameringen M, Mancini C, Wilson C. Buspirone augmentation of selective serotonin reuptake inhibitors (SSRIs) in social phobia. J Affect Disord. 1996;39:115-121.
- 15. Judd LL, Kessler RC, Paulus MP, et al. Comorbidity as a fundamental feature of generalized anxiety disorders: results from the National Comorbidity Study (NCS). Acta Psychiatr Scand Suppl. 1998;393:6-11.
- 16. Wittchen HU. Generalized anxiety disorder: prevalence, burden, and cost to society. Depress Anxiety. 2002;16:162-171.
- 17. Belzer K, Schneier FR. Comorbidity of anxiety and depressive disorders: issues in conceptualization, assessment, and treatment. J Psychiatr Pract. 2004;10:296-306.
- 18. Allgulander C, Nilsson B. A nationwide study in primary health care: one out of four patients suffers from anxiety and depression [in Swedish]. Lakartidningen. 2003;100:832-838.
- 19. Goodman WK. Selecting pharmacotherapy for generalized anxiety disorder. J Clin Psychiatry. 2004;65(suppl 13):8-13.
- 20. Gelenberg AJ, Lydiard RB, Rudolph RL, et al. Efficacy of venlafaxine extended-release capsules in nondepressed outpatients with generalized anxiety disorder: a 6-month randomized controlled trial. JAMA. 2000;283:3082-3088.
- 21. Goodman WK, Bose A, Wang Q. Treatment of generalized anxiety disorder with escitalopram: pooled results from double-blind, placebo controlled trials. J Affect Disord. 2005;87:161-167.
- 22. Ashton H. Benzodiazepine withdrawal: an unfinished story. Br Med J (Clin Res Ed). 1984;288:1135-1140.
- 23. Ashton H. Benzodiazepine withdrawal: outcome in 50 patients. Br J Addict. 1987;82:665-671.
- 24. Ashton H. Protracted withdrawal syndromes from benzodiazepines. J Subst Abuse Treat. 1991;8:19-28.
- 25. Ashton H. The treatment of benzodiazepine dependence. Addiction. 1994;89:1535-1541.
- 26. Ashton H. Guidelines for the rational use of benzodiazepines. When and what to use. Drugs.1994;48:25-40.
- 27. Brewin CR, Andrews B, Rose S. Fear, helplessness, and horror in posttraumatic stress disorder: investigating DSM-IV criterion A2 in victims of violent crime. J Trauma Stress. 2000;13:499-509.
- 28. Dohrenwend BP, Neria Y, Turner JB, et al. Positive tertiary appraisals and posttraumatic stress disorder in US male veterans of the war in Vietnam: the roles of positive affirmation, positive reformulation, and defensive denial. J Consult Clin Psychol. 2004;72:417-433.
- 29. Marshall RD, Olfson M, Hellman F, et al. Comorbidity, impairment, and suicidality in subthreshold PTSD. Am J Psychiatry. 2001;158:1467-1473.
- 30. Ruscio AM, Ruscio J, Keane TM. The latent structure of posttraumatic stress disorder: a taxometric investigation of reactions to extreme stress. J Abnorm Psychol. 2002;111:290-301.
- 31. Marshall RD, Galea S, Kilpatrick D. Psychiatric consequences of September 11. JAMA. 2002;288:2683-2685.
- 32. Marshall RD. Insights into depression and anxiety: overview of the anxiety disorders. Psychiatr Times. 2005;8(suppl):1-8.
- 33. Marshall RD, Beebe KL, Oldham M, Zaninelli R. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry. 2001;158:1982-1988.
- 34. Connor KM, Sutherland SM, Tupler LA, et al. Fluoxetine in post-traumatic stress disorder. Randomised, double-blind study. Br J Psychiatry.1999;175:17-22.
- 35. Davidson J, Baldwin D, Stein DJ, et al. Treatment of posttraumatic stress disorder with venlafaxine extended release: a 6-month randomized controlled trial. Arch Gen Psychiatry. 2006;63:1158-1165.
- 36. Londborg PD, Hegel MT, Goldstein S, et al. Sertraline treatment of posttraumatic stress disorder: results of 24 weeks of open-label continuation treatment. J Clin Psychiatry. 2001;62:325-331.
- 37. Gelpin E, Bonne O, Peri T, et al. Treatment of recent trauma survivors with benzodiazepines: a prospective study. J Clin Psychiatry. 1996;57:390-394.
- 38. Mellman TA, Bustamante V, David D, Fins AI. Hypnotic medication in the aftermath of trauma. J Clin Psychiatry. 2002;63:1183-1184.









