

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Verruca Vulgaris, Molluscum Contagiosum, and Dermatophyte Infection in a Wrestler and Brown Recluse Spider Bite
A 16-year-old boy presents for evaluation of various lesionsthat have appeared on his extremities since he joined thewrestling team 2 months earlier. He is otherwise healthyand takes no medications.
Case 1:



Click to Enlarge
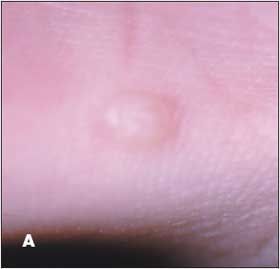
A 16-year-old boy presents for evaluation of various lesions that have appeared on his extremities since he joined the wrestling team 2 months earlier. He is otherwise healthy and takes no medications. Do you recognize these lesions?



Click to Enlarge
A. Verruca vulgaris.
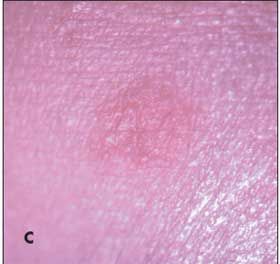
B. Molluscum contagiosum.
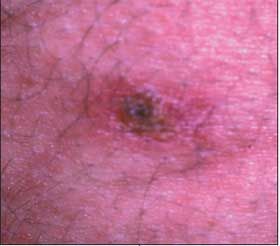
C. Dermatophyte infection.
D. Staphylococcus aureus infection.
E. Herpes simplex. Which of these diseases occur more commonly in wrestlers than in other athletes?


Click to Enlarge


Click to Enlarge
Case 1: This patient had a verruca vulgaris,
A,
molluscum contagiosum,
B,
and a
dermatophyte infection,
C.
These diseases, as well as herpes simplex and
Staphylococcus aureus
infection, occur in wrestlers because of their frequent skin-to-skin contact. There is evidence that intensive exercise combined with weight loss may lower T-cell function in athletes
1
; this effect-in conjunction with the bodily contact, friction, and humid environment of the sport-can heighten participants’ risk of infection. Prophylactic therapy with systemic antiviral agents can prevent outbreaks and, thus, allow athletes to remain in competition. Intermittent prophylactic treatment with a systemic antifungal-despite the absence of FDA approval for such a regimen-has



Click to Enlarge
been prescribed by some physicians. Answer to bonus question: Qualification rules for participation in matches by wrestlers with cutaneous infections differ in each state. Generally, a referee will disqualify a contestant who has an active herpesvirus, dermatophyte, or staphylococcal infection.


Click to Enlarge



A 25-year-old man received a bite on his back 2 days earlier. He killed and recovered a spider he assumed was the culprit. A truncal rash, malaise, a low-grade fever, and aches developed the next day. The patient brings the crushed spider with him to the emergency department. The rash on the patient’s trunk was caused by the bite of a . . .
Click to Enlarge


Click to Enlarge
A. Brown recluse spider.
B. Wood tick.
C. Black widow spider.
D. Deer tick.
E. Wolf spider.
F. Orb weaver.
Bonus questions: In which region of the United States are brown recluse spiders endemic? Which region has the highest incidence of Rocky Mountain spotted fever?



Click to Enlarge
Case 2:
The
brown recluse spider (Loxosceles laeta),
A,
was identified by the characteristic violin shape on its back. The arthropod’s bite caused a maculopapular rash, fever, malaise, aches, chills, and sweats. This presentation is not typical; brown recluse spider bites are rarely associated with systemic symptoms. The patient was given dapsone. The rash and other symptoms cleared in 2 days, and the site of the bite healed without further intervention in 2 weeks.
1
Black widow spiders have a red hourglass shape on the abdomen. Their bites cause severe abdominal pain, cramps, vomiting, and chills-symptoms that are often mistaken for food poisoning. The bite of wolf spiders and orb weavers can produce a local reaction but generally do not cause systemic symptoms. The rash on the patient’s trunk is not typical of Rocky Mountain spotted fever, which is transmitted by wood ticks, or of Lyme disease, which is transmitted by deer ticks. Answers to bonus questions: In this country, brown recluse spiders are endemic in the south and the central midwest.
2
Rocky Mountain spotted fever is most prevalent in the south Atlantic region.
3
REFERENCES:
1.
Rees R, Campbell D, Rieger E, King LE. The diagnosis and treatment of brown recluse spider bites.
Ann Emerg Med.
1987;16:945-949.
2.
Vetter RS, Bush SP. Reports of presumptive brown recluse spider bites reinforce improbable diagnosis in regions of North America where the spider is not endemic.
Clin Infect Dis.
2002;35:442-445.
3.
Treadwell TA, Holman RC, Clarke MJ, et al. Rocky Mountain spotted fever in the United States, 1993-1996.
Am J Trop Med Hyg.
2000; 63:21-26.
Case 3:



Click to Enlarge
An otherwise healthy 16-year-old girl awoke 2 days earlier with an extremely painful ulcer on her right labia. She has no other mucosal or cutaneous lesions. There is no history of trauma, preceding infection, or exposure to irritants or allergens. The patient is a member of the track team; she denies being sexually active. Which condition in the differential is the likely diagnosis?
A.
Herpes simplex.
B.
Chancre.
C.
Chancroid.
D.
Brown recluse spider bite.
E.
Factitial dermatitis.
Your initial approach is to . . .
F.
Perform a viral culture.
G.
Perform a bacterial culture.
H.
Perform a biopsy.
I.
Order a rapid plasma reagin test.
J.
Offer reassurance, provide conservative management with antibiotic ointment, and observe closely for the next 2 weeks.



Click to Enlarge
Case 3:
This patient’s painful ulcerative lesion is a classic presentation of a
brown recluse spider bite,
D;
the actual bite from a spider hidden in the patient’s underwear was painless. Two days after therapy with dapsone was initiated, the patient’s pain eased significantly; complete healing without scarring was noted 4 weeks later. A rapid plasma reagin test,
I,
ruled out syphilis, which usually starts as an asymptomatic papule that forms an ulcer, or chancre, over several days. Typically, chancroid-a disease seen more commonly in men than in women-presents as a painful pustule that develops into a painful ulcer. Herpes simplex virus infections usually feature grouped vesicles that form tender or pruritic shallow erosions. A factitial lesion is a diagnosis of exclusion. When the diagnosis is in doubt, cultures can rule out infections and a biopsy may be needed.
Case 4:



Click to Enlarge
The asymptomatic white spots on the arms of a 46-year-old woman have been present for 2 years. She enjoys gardening and other outdoor activities. The patient has taken hormone replacement therapy for the past 3 years. Which condition in the differential is the likely cause?
A.
Vitiligo.
B.
Tinea versicolor.
C.
Guttate hypomelanosis.
D.
Factitial dermatitis.
E.
An adverse drug reaction.



Click to Enlarge
Case 4:
Guttate hypomelanosis,
C,
is seen commonly on the forearms and shins of women who are older than 40 years. The condition is attributable to longterm sun exposure. The depigmentation that is characteristic of vitiligo has a predilection for periorifacial and/or genital areas. Tinea versicolor, which is associated with scale, usually arises on the trunk. Some healed factitial lesions feature depigmentation caused by scarring, which was absent on this patient. Cutaneous drug reactions are usually more diffuse than this patient’s rash; in addition, hormone replacement agents are not photosensitizing.












