

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Mycobacterium marinum Granuloma in a Fisherman
While fishing in the Chesapeake Bay, an 81-year-old man slipped and fell into the water. Afterward, he noticed a superficial abrasion over his right knee. During the next 10 days, red bumps, pustules, and slight tenderness developed. He was treated empirically with mupirocin ointment, amoxicillin/clavulanate and subsequently with cephalexin. However, new papular lesions continued to develop adjacent to the area of involvement, which showed no signs of healing.
While fishing in the Chesapeake Bay, an 81-year-old man slipped and fell into the water. Afterward, he noticed a superficial abrasion over his right knee. During the next 10 days, red bumps, pustules, and slight tenderness developed. He was treated empirically with mupirocin ointment, amoxicillin/clavulanate and subsequently with cephalexin. However, new papular lesions continued to develop adjacent to the area of involvement, which showed no signs of healing.
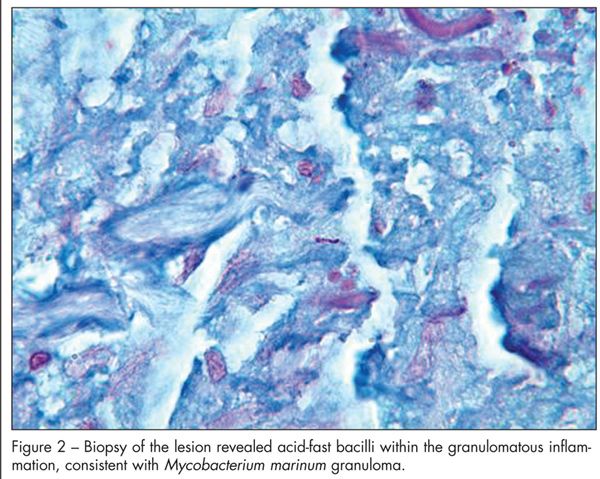
Eight weeks after the injury, the patient presented with a 3 X 4-cm patch of densely packed 0.5- to 1.5-mm papules with background erythema (Figure 1). A wedge incisional biopsy was performed. One-half of the specimen was sent for histopathological examination, including periodic acid- Schiff and acid-fast bacillus (AFB) stains. Results showed necrotizing granulomatous inflammation of the superficial and deep dermis with associated ulceration and AFB within the granulomatous inflammation, consistent with Mycobacterium marinum granuloma (Figure 2).
The other half of the specimen was sent for bacterial, fungal, and atypical mycobacteria cultures; however, these were not completed because of a processing error in the laboratory.


Treatment with minocycline (100 mg PO bid for 6 weeks) led to complete resolution without any recurrence 6 months later.
DIAGNOSIS OF CHRONIC LOCAL INFECTIONS
When evaluating a chronic lesion, it is important to document its progression and the patient’s medical and travel history, current medications, and animal and environmental exposures. Less common pathogens are associated with immunocompromised states, human or animal bites, international travel, and certain environmental agents (such as water or soil). In these cases, empiric therapy may not be appropriate.
SORTING THROUGH THE DIFFERENTIAL
The presentation and failure of resolution in this patient strongly suggested a chronic infection caused by a resistant or unusual pathogen. M marinum infection was the logical diagnosis in view of the history of trauma in an open body of water.
M marinum also causes fish tank granuloma on the hands of aquarium owners. About 2 to 8 weeks after inoculation, a solitary papule forms that often progresses to a granulomatous nodule or multiple papules. The lesions may ulcerate or expand into an enlarging localized plaque.1 This infection also has a predilection to spread along lymphatic drainage pathways in a characteristic sporotrichoid pattern.
Tissue culture for acid-fast organzisms can confirm the diagnosis. Although histological examination and special stains are generally less sensitive, they did provide a definitive diagnosis in this case. Treatment with tetracycline, doxycycline, minocycline, trimethoprim/sulfamethoxazole, rifampin, or ethambutol is effective; however, a prolonged course of up to 6 months is necessary.2
Other infectious causes that present similarly to M marinum infection were considered, including:
•Sporothrix schenckii, a dimorphic fungus found globally in soil and plant debris. The usual route of infection is traumatic implantation by splinters or thorns, hence the term “rose gardener disease.”3 After inoculation, a small nodule forms that enlarges and ulcerates. Papules and nodules can develop proximal to the site of inoculation and may follow a sporotrichoid pattern.
•Nocardiosis, which is caused by a gram-positive, filamentous, acid-fast bacteria and presents as tender subcutaneous nodules and nonhealing ulcers after traumatic inoculation with contaminated soil.4
•Leishmaniasis, which is caused by an intracellular protozoan; it affects millions worldwide and is becoming more frequent in the United States because of international travel and military missions. The infection presents as an erythematous papule that enlarges over several weeks and eventually ulcerates. Weeks to months later, it resolves, leaving a disfiguring scar.5
•Tularemia, a disease caused by the gram-negative coccobacillus Francisella tularensis, which also causes a chronic infection at the site of inoculation; however, it is usually seen in hunters who skin rabbits.6
Allergic contact dermatitis from mupirocin used to treat the abrasion was also considered; however, the patient’s lesion was tender and never pruritic. Localized pustular psoriasis, segmental lichen planus, and lichen simplex chronicus were excluded by the history. Chronic herpes simplex infection was not suspected because the patient was immunocompetent. Methicillin-resistant Staphylococcus aureus and gram-negative organisms would have been expected to demonstrate more suppuration than was evident here.
DIAGNOSTIC CONFIRMATION WITH TISSUE SAMPLING
In patients with an unusual history/presentation or extended duration of a skin infection, a definitive diagnosis can be made with a simple punch or deep “saucerization” shave biopsy. However, a wedge incision may be performed, as in this case. The biopsy specimen can be divided with half placed in a sterile container for tissue culture and half placed in formaldehyde for histopathological examination.
Always send a thorough history with ordered differential diagnosis to the pathologist so that he or she is prompted to order appropriate stains. On the requisition, indicate whether tissue culture is to be performed and specify whether aerobic or anaerobic bacterial cultures are needed and, especially, when to test for Nocardia, fungal, and acid-fast organisms. Nocardia, because it is a slow-growing organism, requires that culture plates be incubated longer than the standard 48 hours.4 Viral culture techniques must also be specified if chronic herpes simplex is suspected.
References:
REFERENCES:
1.
Kullavanijaya P. Atypical mycobacterial cutaneous infection.
Clin Dermatol.
1999;17:153-158.
2.
Jogi R, Tyring SK. Therapy of nontuberculous mycobacterial infections.
Dermatol Ther.
2004;17: 491-498.
3.
Tobin EH, Jih WW. Sporotrichoid lymphocutaneous infections: etiology, diagnosis and therapy.
Am Fam Physician.
2001;63:326-332.
4.
Bhalodia AM, Lertzman BH, Kantor GR, Granick MS. Localized cutaneous Nocardia brasiliensis mimicking foreign body granuloma.
Cutis.
1998;61: 161-163.
5.
Markle WH, Makhoul K. Cutaneous leishmaniasis: recognition and treatment.
Am Fam Physician.
2004; 69:1455-1460.
6.
Hayes E, Marshall S, Dennis D. Tularemiaâ United States, 1990-2000.
Arch Dermatol.
2002; 138:988-989.
http://archderm.ama-assn.org/cgi/ content/full/138/7/988/
. Accessed August 5, 2009.













