

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Academic Detailing: Focus Is on Appropriate Care
The practice of academic detailing is gaining interest and momentum in some health care circles. The primary aim of academic detailing is to prevent the overuse and misuse of certain medications. This is done by educating prescribers on the therapies that are clinically appropriate as well as the costs of therapeutically similar choices. It is less an issue of switching to generics than it is of favoring step therapy or moving toward cost-effective therapeutically equivalent options. A well-designed program should maintain prescriber autonomy and quality of care while helping manage drug costs for both health plans and patients.
The practice of academic detailing is gaining interest and momentum in some health care circles. The primary aim of academic detailing is to prevent the overuse and misuse of certain medications. This is done by educating prescribers on the therapies that are clinically appropriate as well as the costs of therapeutically similar choices. It is less an issue of switching to generics than it is of favoring step therapy or moving toward cost-effective therapeutically equivalent options. A well-designed program should maintain prescriber autonomy and quality of care while helping manage drug costs for both health plans and patients.
How do such programs work?
Academic detailing programs typically have a field staff that not unlike detailers for pharmaceutical manufacturers, calls on physicians who are high-volume prescribers of medications whose costs are selected for management under the program. Academic detailers have backgrounds in nursing, pharmacy, and pharmacology. Some programs have used physicians as detailers,1-3 but that increases the cost of such programs.
One of the most comprehensive programs is the Independent Drug Information Service (iDiS) in Pennsylvania, in which trained persons meet with physicians throughout the state. The program's goal is "to improve appropriateness of prescribing by providing unbiased, noncommercial, evidence-based, and timely information to prescribers."4
The program is administered by the Pennsylvania Office of Health Care Reform. Clinical direction is provided by consultants at Harvard Medical School in Boston,4 who have trained a team of clinicians in Pennsylvania on academic detailing, drug classes selected and rationale, and the message to communicate to prescribers.
The Pennsylvania initiative grew out of a desire to implement sound policies for coverage of prescription drugs across all of the state's programs.4 The iDiS replaced a point-of-sale prospective audit that rejected claims for certain medications not on the state's preferred list.
How are targeted drugs selected?
A comment made frequently by program leaders is that academic detailing is not about not prescribing a particular drug because of cost. Instead, they say, it is about targeting certain categories of drugs that have the potential for overutilization or inappropriate use, drugs for which it was felt the physicians needed to have medical evidence regarding when and when not to prescribe.
The Pennsylvania program targets prescribing practices in 6 therapeutic classes, including cyclooxygenase-2 and proton pump inhibitors.
Does this approach really work?
Available evidence suggests that academic detailing has had an impact on prescribing habits. For example, Simon and colleagues1 reported on prescribing changes for antihypertensive drugs in a large HMO following academic detailing. They compared 3 methodologies: group detailing, individual detailing, and the usual standard of care without detailing (in which prescribers received practice guidelines in the mail).
They studied the prescribing patterns of antihypertensive medications for patients with newly diagnosed hypertension who were receiving treatment at 1 of 9 clinical sites of the HMO. The researchers randomly assigned 3 practice sites to receive group detailing (227 prescribers), 3 to individual detailing (235 prescribers), and 3 to usual care (319 prescribers). In the first year following academic detailing, absolute rates of use of diuretics or β-blockers (promoted by the academic detailers) increased by 13.2% in the group-detailing practices, 12.5% in the individual-detailing practices, and 6.2% in the usual-care practices.
Another study demonstrated that distribution of guidelines without any personal contact did not appear to have any impact on prescribing.2
Whether the effect of academic detailing is lasting appears to depend on the approach used to influence prescribing. In the Simon study,1 at 2 years after detailing, use of guideline-recommended medications over baseline was greater with individual-detailing practices (14.7%) than with group-detailing practices (11.3%) or usual-care practices (10.1%). This suggests a persistent effect of individual detailing but not group detailing. However, neither type of academic detailing had a clinically meaningful effect on blood pressure control, so there was no negative impact on quality of care. However, it appears that to achieve a sustained impact on prescribing, the message needs to be repeated.
Is the purpose of the program to save money?
Saving money is not the only reason for an academic detailing program. The literature on academic detailing emphasizes support for quality care as the main mission of the program. The educational focus is on appropriateness of care and, unlike pharmaceutical industry detailing, is not aimed to boost marketing or sales of drugs.
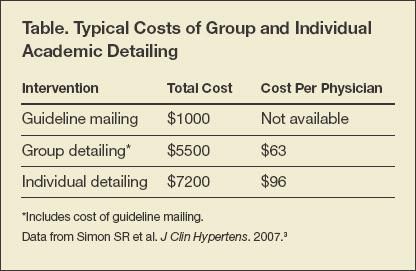
Another study by Simon and colleagues3 estimated the costs and cost savings of implementing an academic detailing program as described above from a plan or payer perspective. The costs and cost savings in the group- and individual-detailing arms were compared with the standard-of-care arm that only received guidelines in the mail. The mean detailing time for individual sessions was 30 minutes (range, 10 to 90 minutes), including travel time to the physician's office and time spent waiting to see the physician. Group sessions lasted 60 minutes.
The total costs of each intervention are shown in the Table. Not surprisingly, the costs for individual intervention were highest. For all patients with incident hypertension in the study's individual detailing arm, the annual total drug cost savings were estimated at $21,711 (95% confidence interval, $9709 to $53,131). The authors suggested that the results might provide guidance to health plans on the costs of academic detailing interventions to change prescribing patterns.


If the purpose is not to save money, what is the value of academic detailing?
The consensus among academic detailing program managers and managed care executives is that academic detailing has value as an active method of influencing prescribing habits, distinct from passive methods of restricted formularies, preferred or tiered drug lists, rejection of claims, or prior authorization programs.
In some cases, academic detailing programs can be used to influence adoption of best practices. In a recent initiative in New York City, 2 health educators were trained in the latest guidelines and evidence-based data for breast cancer screening to increase the number of women in an inner-city setting who received screening.5 After academic detailing, significant increases were seen in physicians' knowledge of current screening guidelines and in the number of women in the target population who were screened for breast cancer.
Where are academic detailing programs in place?
In the United States, active programs exist in Pennsylvania and Vermont, and recently the state of Maine enacted legislation establishing a statewide academic detailing initiative.6 Academic detailing is also practiced in Australia7 (run by the National Prescribing Service) and throughout Europe.
Do these programs use incentives?
Pharmaceutical company detailers typically use incentives to gain an audience with a physician. With academic detailing, "knowledge is the main incentive," according to the iDiS program.4 The program in Australia notes that physician compensation is available for participation in some of its activities but does not provide details.7 One program manager noted its academic detailers will provide lunch at the physician's office as is commonly done by pharmaceutical manufacturer detailers if asked to do so.
Is participation voluntary?
Prescriber participation is generally voluntary as it is for iDiS4 and the Vermont program.8 However, this could change. For example, as large HMOs implement such programs, participating could become a requirement of re-credentialing or of health plan participation. More important, academic detailing activities have been linked to quality improvement initiatives.9,10 Others have described academic detailing as a component of e-prescribing and electronic health records to reduce inappropriate medication use.11 Another possibility is that continuing education credits could be incorporated into this type of program.
How much does a program cost to operate?
There is no simple answer to this question. It depends on the type of program and the program's offerings (eg, frequency of visits, individual or group detailing, staffing). The Pennsylvania program costs about $80,000 a month. Program managers note that the state spends $3 billion a year on prescription drugs through all of its programs, including Medicaid, the Program for All-inclusive Care for the Elderly, and the state employee retiree program.
Are there any programs that address HIV care specifically?
There are no HIV-specific academic detailing programs in the United States. The Australian program does address HIV medicine with fact sheets on antiretroviral drugs and sponsored conferences on managing HIV care.11
As persons with HIV/AIDS live longer, it becomes necessary to treat diseases of aging as well as the long-term effects of HIV infection and antiretroviral treatment. These include hypertension, cardiovascular disease, and the lipid and metabolic disorders often seen in HIV/AIDS patients.
Although there are essentially no generic versions of antiretrovirals available for use in the United States, this may change. Significant numbers of HIV-infected persons are cared for in publicly funded programs (eg, Medicaid, the Ryan White CARE Act, and Medicare), and many states have demonstration projects under way for Medicaid managed care enrollees.
Conclusion
Restricted formularies are a fact of life in managed care and publicly funded programs. The usual driver of formulary restriction is cost. A passive approach to drug utilization management is the restricted or tiered drug list. Prior authorization requirements are often part of drug utilization management.
An active approach, such as academic detailing, that manages the costs of prescription medication programs allows prescribers to retain the flexibility to respond to individual patient needs. It is all about maintaining the quality of care for patients.
References:
References
- 1. Simon SR, Majumdar SR, Prosser LA, et al. Group versus individual academic detailing to improve the use of antihypertensive medications in primary care: a cluster-randomized controlled trial. Am J Med. 2005;118:521-528.
- 2. Wong RY, Lee PE. Teaching physicians geriatric principles: a randomized control trial on academic detailing plus printed materials versus printed materials only. J Gerontol A Biol Sci Med Sci. 2004;59:1036-1040.
- 3. Simon SR, Rodriguez HP, Majumdar SR, et al. Economic analysis of a randomized trial of academic detailing interventions to improve use of antihypertensive medications. J Clin Hypertens. 2007;9:15-20. www.blackwell-synergy.com/doi/full/10.1111/j.1524-6175.2006.05684. x?CFID=3292019&CFTOKEN=92040028. Accessed January 22, 2008.
- 4. Independent Drug Information Service. www.rxfacts.org. Accessed January 22, 2008.
- 5. Gorin SS, Ashford AR, Lantigua R, et al. Effectiveness of academic detailing on breast cancer screening among primary care physicians in an underserved community. J Am Board Fam Med. 2006;19:110-121. www.medscape.com/viewarticle/524582. Accessed January 22, 2008.
- 6. State of Maine Legislature. An Act to Establish a Prescription Drug Academic Detailing Program. http://janus.state.me.us/legis/LawMakerWeb/externalsiteframe.asp?ID=280023464&LD=839 & Type=1&SessionID=7. Accessed January 22, 2008.
- 7. National Prescribing Service. Australia. www.nps.org.au. Accessed January 22, 2008.
- 8. University of Vermont College of Medicine. Office of Primary Care. Academic Detailing: Reforming Medication Prescribing Practices. www.med.uvm.edu/ahec/TB1+BL.asp?SiteAreaID=290. Accessed January 22, 2008.
- 9. Goldberg HI, Wagner EH, Fihn SD, et al. A randomized controlled trial of CQI teams and academic detailing: can they alter compliance with guidelines? Jt Comm J Qual Improv. 1998;24:130-142.
- 10. Brown JB, Shye D, McFarland BH, et al. Controlled trials of CQI and academic detailing to implement a clinical practice guideline for depression. Jt Comm J Qual Improv. 2000;26:39-54.
- 11. Simon SR, Smith DH, Feldstein AC, et al. Computerized prescribing alerts and group academic detailing to reduce the use of potentially inappropriate medications in older people. J Am Geriatr Soc. 2006;54:963-968.





Common Side Effects of Antiretroviral Therapy in HIV Infection
February 7th 2013What are some of the more common side effects of antiretroviral therapy, and what can the primary care physician do to help manage these effects? In this podcast, infectious disease expert Rodger MacArthur, MD, offers insights and points readers to updated comprehensive guidelines.



