

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Tracheal Stenosis After Prolonged Intubation in an Adult Male


Figure 1. In-office spirometry tracing.
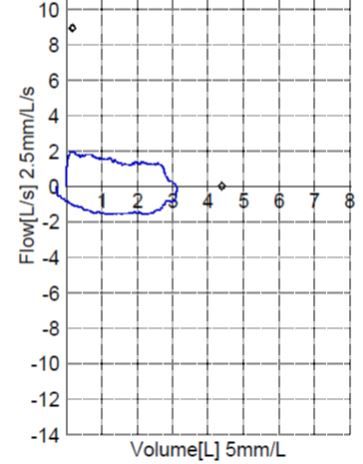


Figure 2. Tracheal stenosis before surgery.
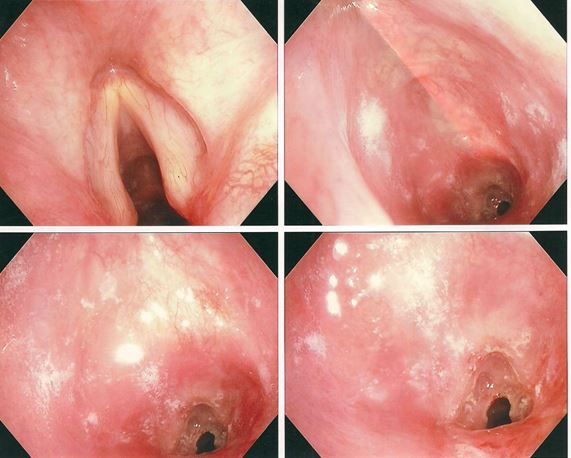


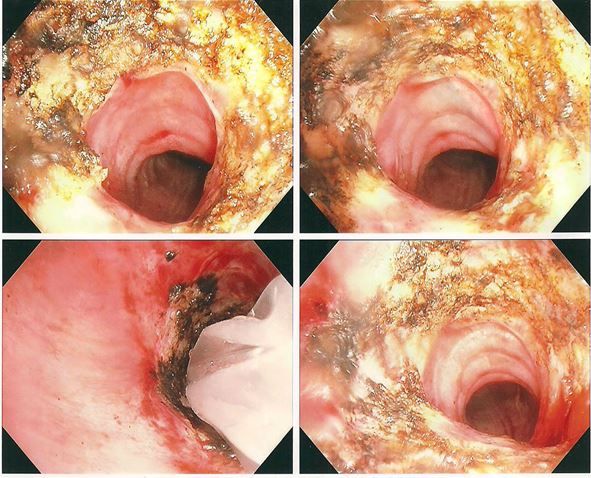
Figure 3. Tracheal stenosis repair with laser surgery.
A 56-year-old man, Mr A, comes to your office 6 weeks after a long hospitalization for severe pancreatitis secondary to gallbladder disease. During that admission, acute respiratory distress syndrome and respiratory failure developed and the patient was intubated for 9 days. A large pancreatic fluid collection also developed while he was hospitalized and has caused noticeable abdominal swelling and pain. Since his hospital discharge, he has noticed worsening shortness of breath, which has increased markedly over the past week, with associated wheezing. He has no previous history of COPD or asthma and has never smoked cigarettes.
On physical examination, you note wheezing throughout his chest, and he is in moderate respiratory distress. You perform spirometry, which produces the flow volume loop shown in Figure 1. (Click figures to enlarge.)
Question 1: What does the flow volume loop show?
A. Obstructive pattern
B. Restrictive pattern
C. Normal pattern
D. Variable expiratory upper airway obstruction
E. Fixed upper airway obstruction
Question 2: What is the most likely cause of this patient’s dyspnea?
A. Deconditioning from previous illness
B. Adult-onset asthma
C. Cardiac asthma
D. Tracheal stenosis from prolonged intubation
Answers:
Question 1: E. Fixed upper airway obstruction
Question 2: D. Tracheal stenosis from prolonged intubation
Discussion
The flow volume loop shows a flattening of both the expiratory and inspiratory flows in a pattern consistent with a fixed upper airway obstruction, such as would be seen in a patient with tracheal stenosis secondary to scar formation after a prolonged intubation.
Mr A was referred immediately to a thoracic surgeon, who admitted the patient. He found that the tracheal lumen was narrowed to 4 mm in diameter by tracheal scar tissue (Figure 2) and performed successful laser surgery on the obstruction (Figure 3). (Images shown are representative.)
Tracheal stenosis can occur after prolonged intubation and is believed to be caused by the cuff of the endotracheal tube eroding the mucosa of the laryngeal airway. Necrosis and distortion of the mucosa occur, followed by progressive scarring. Shortness of breath typically occurs within 5 weeks of injury. The associated stridor is suggestive of this injury, but may be mistaken for wheezing.
Pulmonary function testing typically reveals a fixed upper airway obstruction pattern, but bronchoscopy or CT scanning is necessary for definitive diagnosis. Tracheal stenosis can be treated by a variety of techniques, depending on local expertise, including resection, stenting, or ablation with lasers or other devices.








")


