

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Stop and Catch Your Breath: A Respiratory Photo Essay
Pulmonary edema, tracheal stenosis, pulmonary embolism, pulmonary sarcoidosis, respiratory bronchiolitis interstitial lung disease, giant bullous emphysema-a close look at a variety of troublesome lung conditions.



Case 1:
A 73-year-old woman was admitted with a 1-week history of worsening shortness of breath and bleeding from a new left breast mass. She had a history of hypertension and type 2 diabetes mellitus. She was afebrile, hypertensive, tachycardic, and dyspneic on rest.
A breast examination showed an ulcerated and necrotic mass in the left breast that involved the nipple. There were multiple palpable, hard and fixed lymph nodes in the bilateral axillae and supraclavicular areas. There was dullness to percussion over both sides of the chest posteriorly.
A chest radiograph showed moderate to large bilateral pleural effusions. A new chest radiograph showed diffuse infiltrates over bilateral lower lung fields, consistent with re-expansion pulmonary edema (REPE), a type of noncardiogenic pulmonary edema that follows re-expansion of the lung after performing thoracentesis for large amounts of pleural effusion or pneumothorax.
Pathophysiologic mechanisms include increased permeability of the pulmonary capillaries resulting from inflammation, increased pulmonary hydrostatic pressure caused by enhanced venous return, altered lymphatic clearance, and decreased amounts of functional surfactant. Clinical features of REPE include chest discomfort, persistent cough, tachypnea, tachycardia, and worsening hypoxemia that may be refractory to oxygen therapy. Diagnosis usually is based on the characteristic serial radiographic features.
Case and image provided by Ranjita Pallavi, MD and Hossam Amin, MD
NEXT CASE »
For the discussion, click here.


Case 2:
A 56-year-old man comes to your office 6 weeks after a long hospitalization for severe pancreatitis secondary to gallbladder disease. Acute respiratory distress syndrome and respiratory failure had developed, and he was intubated for 9 days. A large pancreatic fluid collection that also developed has caused noticeable abdominal swelling and pain. Since his discharge, he has noticed worsening shortness of breath with associated wheezing.
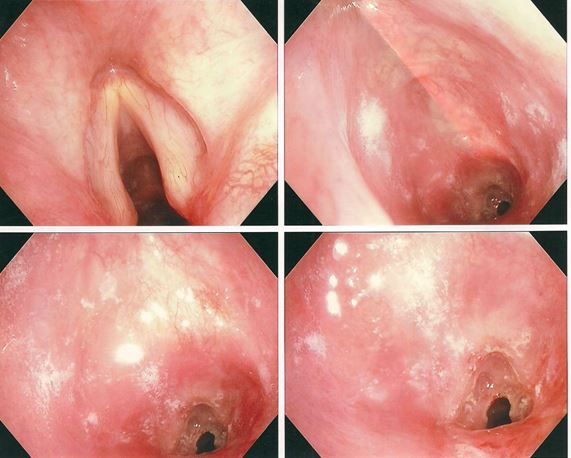
The patient is in moderate respiratory distress. Spirometry shows a flattening of both the expiratory and inspiratory flows in a pattern consistent with a fixed upper airway obstruction, such as would be seen in a patient with tracheal stenosis secondary to scar formation after a prolonged intubation. A thoracic surgeon found that the tracheal lumen was narrowed to 4 mm in diameter by tracheal scar tissue and performed successful laser surgery on the obstruction.
Tracheal stenosis can occur after prolonged intubation; it is thought to be caused by the cuff of the endotracheal tube eroding the mucosa of the laryngeal airway. Necrosis and distortion of the mucosa occur, followed by progressive scarring. Shortness of breath typically occurs within 5 weeks of injury. Associated stridor, suggestive of this injury, may be mistaken for wheezing.
Pulmonary function testing typically reveals a fixed upper airway obstruction pattern, but bronchoscopy or CT scanning is necessary for definitive diagnosis.
Case and image provided by Jonathan Ilowite, MD
NEXT CASE »
For the discussion, click here.


Case 3:
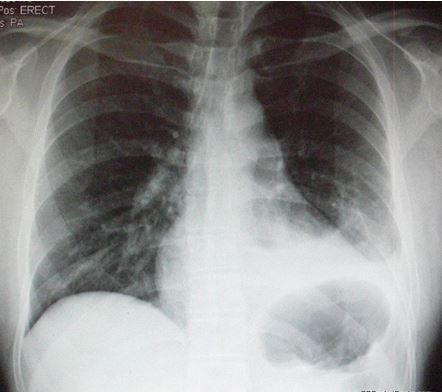
A 29-year-old male presents to the ED with dyspnea and pleuritic chest pain. He had been hospitalized for a stab wound to the chest and required a chest tube for a hemopneumothorax. He had been improving, but then his symptoms suddenly worsened. He has decreased breath sounds on the symptomatic left side, the side on which he sustained the stab wound.
With suspicion of a recurrent pneumothorax, this chest x-ray film is ordered. It shows scarring and a small residual hemothorax on the left, explaining the decreased breath sounds. The radiologist reads it as negative for pneumothorax.
Given a recent hospitalization and surgical procedure, the patient has risk factors for pulmonary embolism (PE). A chest CT scan was read as positive for PE.
PE classically presents with pleuritic chest pain and dyspnea in a patient with known risk factors and no other explanation for the symptoms. However, PEs often do not present classically.
Clinical tools that can help discern which patients require a workup for PE include known risk factors for PE and historical and physical examination findings that may suggest PE.
Case and image courtesy of Brady Pregerson, MD
NEXT CASE »
For the discussion, click here.


Case 4:
A 44-year-old African American woman was evaluated for symptoms of worsening cough, shortness of breath, chest tightness, and fatigue of 6 months’ duration. Bronchial asthma had been her diagnosis 2 years earlier, and she had been compliant with her inhalation therapy.
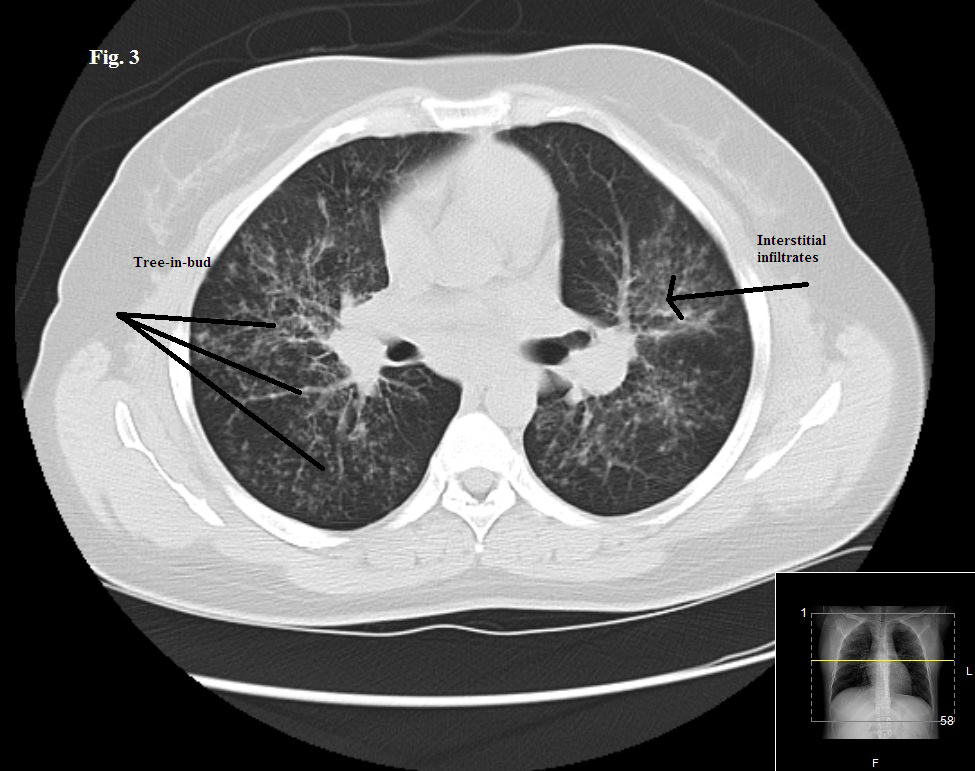
The physical exam showed bilateral diffuse wheezing and crackles. An earlier chest radiograph showed mild hilar prominence. A repeated radiograph showed new bilateral diffuse interstitial infiltrates involving both lungs and bilateral hilar lymphadenopathy. This chest CT scan showed similar findings with a tree-in-bud appearance predominantly in the midlung zones and perihilar areas. Pulmonary function testing results showed a progression from moderate to severe obstructive lung disease and worsening diffusing capacity of the lung for carbon monoxide.
Positive findings of sarcoidosis involving the skin along with bilateral diffuse interstitial lung infiltrates and hilar lymphadenopathy supported a diagnosis of pulmonary sarcoidosis.
Sarcoidosis affects the lungs in 90% of cases. It usually involves the intrathoracic lymph nodes and, less frequently, the lung parenchyma. Up to 50% of patients have symptoms similar to those of asthma, such as cough, wheezing, dyspnea, chest pain, chest tightness, and fatigue.
Case and image courtesy of Ranjita Pallavi, MD and Hossam Amin, MD
NEXT CASE »
For the discussion, click here.



Case 5:
A 43-year-old African American woman presented with severe dyspnea, wheeze, and cough productive of white sputum. Years earlier, she had a diagnosis of asthma based on symptoms of wheeze and cough. On examination, she was in extremis, sitting upright in bed, using accessory respiratory muscles, and unable to complete sentences because of severe dyspnea.
Chest auscultation revealed bilateral diffuse coarse crackles and wheeze. A chest radiograph showed prominence of the interstitial markings. A CT scan of the chest revealed bilateral, diffuse, ground-glass opacities without significant air trapping. Bronchoscopy was performed.
A low-power view of the biopsy specimen showed a terminal and a respiratory bronchiole surrounded by scar tissue and alveolar septal thickening. The presence of brown pigmented macrophages abundant in the airspace adjacent to the affected bronchioles led to a diagnosis of respiratory bronchiolitis interstitial lung disease (RB-ILD).
A rare interstitial lung disease, RB-ILD is almost always associated with a history of smoking. RB-ILD may represent a progression of smoking-related respiratory bronchiolitis (smokers’ bronchiolitis), a very common asymptomatic histopathological finding. The distinction between smokers’ bronchiolitis and RB-ILD lies in the onset of symptoms and biopsy findings of interstitial inflammation and/or fibrosis.
Case and image provided by Nirav P. Patel, MD, MPH
NEXT CASE »
For the discussion, click here.



Case 6:
A 54-year-old man presented to the ED with sudden onset of palpitations. His medical history included stage IV renal cell carcinoma, end-stage COPD, NYHA class IV heart failure, recent pulmonary embolism, and ongoing tobacco abuse. Cardiac examination revealed atrial flutter and a rapid ventricular rate.
A CT scan of the thorax was ordered to help determine whether a recurrent pulmonary embolism may have contributed to the arrhythmia.
The patient also had a more than 20-year history of giant bullous emphysema (GBE). He had undergone a left-sided bullectomy in his 40s to help alleviate symptoms. He has continued to smoke and the disease has progressed.
GBE, or “vanishing lung syndrome,” is a rare condition typically found in young men who smoke. It is caused by paraseptal emphysematous bullae that coalesce and eventually compress the lung parenchyma. By definition, the bullae must occupy at least one-third of the hemithorax and thus can be mistaken for a pneumothorax on a standard chest film.
Case and image provided by Mark Masciocchi, MD, Shashank Jain, MD, and Anthony Donato, MD








")


