

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Reversible Coma in a Young Postpartum Woman
A young woman was admitted at 36 weeks' gestation with severe preeclampsia. During delivery, she experienced generalized seizures. She remained postictal throughout the normal vaginal birth.


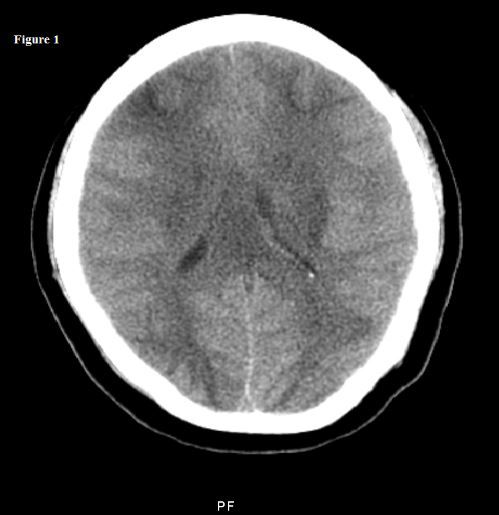
Figure. Click to enlarge.
A 22-year-old pregnant woman presented at 36 weeks of gestation with a 1-day history of mild headache, blurred vision, and epigastric pain. Her blood pressure on admission was 175/120 mm Hg and heart rate 93 beats/min. Urinary protein level was >300 mg on a random sample. She was admitted for severe preeclampia with signs of early labor. Treatment with magnesium sulfate and intravenous labetolol was started. During labor, however, she experienced multiple generalized tonic clonic seizures. She had a normal vaginal delivery but remained postictal throughout. She was intubated for airway protection and put on a mechanical ventilator.
Neurologic exam was notable for withdrawal of all 4 extremities to painful stimuli. Pupils were mid-position fixed and deep tendon reflexes were 2+ with extensor plantar response bilaterally. She had decorticate posturing. Intravenous levetiracetam was started, and she was transferred to the ICU. Brain CT without contrast showed marked diffuse vasogenic cerebral edema (Figure). It also showed partial bilateral uncal herniation and effacement of the suprasellar cistern. Bilateral low attenuation of frontal and occipital lobes was noted. This was most likely the result of marked edema presumed to be related to posterior reversible encephalopathy syndrome (PRES).
In view of uncal herniation, the patient was hyperventilated to lower elevated intracranial pressure and intravenous mannitol was started. Laboratory investigations revealed elevated liver enzyme levels, AST 518 U/L (11-39) and ALT 251 U/L (11-35); platelet count 24,000/µL (150,000-400,000), and decrease in hematocrit 23.4% (37%-47%), with elevated LDH 1676 U/L (100-190), consistent with HELLP syndrome (hemolysis, elevated liver enzymes, and low platelets).
A repeated brain CT performed 12 hours later showed no improvement.
Labetolol and supportive measures including mechanical ventilation were continued and the patient’s mental status improved after 24 hours. She became more alert and responsive and was successfully extubated on the third hospital day. There was significant improvement in all her laboratory parameters. AST decreased to 29 U/L, ALT to 57 U/L, and LDH to 430 U/L. Platelet count improved to 218,000/µL. Hematocrit remained stable. A brain CT performed 1 week later showed that the periventricular white matter changes seen previously had significantly improved with complete resolution of diffuse cerebral edema. The patient recovered completely without any neurologic deficit.
Discussion
The development of focal neurologic deficits in the postpartum period is uncommon and differential diagnoses include seizures, posterior circulation stroke, cerebral venous thrombosis, complicated migraine, eclampsia, encephalitis, vasculitis, cerebral artery dissection, and posterior reversible encephalopathy syndrome (PRES).
Hinchey et al2 first reported a case of reversible posterior leukoencephalopathy syndrome in 1996, but in 2000 the name was changed to PRES. The reported incidence of PRES is approximately 0.01%.3 PRES is a cliniconeuroradiologic entity. Clinical features include headache, confusion, seizures, cortical visual disturbances, and altered metal status. The radiologic findings include bilateral white and gray matter changes that predominantly affect the posterior cerebral hemispheres.
Common causes include hypertension, preeclampsia/eclampsia, uremia, immunosuppressive drugs, transplantation (both solid organ and allogenic bone marrow), and systemic lupus erythematosus. Patients often have weakness and limb ataxia, and deep tendon reflexes are brisk. Theories proposed regarding its pathophysiology include disruption of the blood-brain barrier related to accelerated hypertension; endothelial dysfunction caused by circulating toxins in patients with sepsis; preeclampsia and autoimmune disorders; and ischemic edema secondary to focal vasospasm and blood flow decrement.1 Eclamptic patients with atypical features such as focal neurologic deficits, markedly depressed mental status, and profound visual disturbances should be evaluated by neuroimaging.
A CT scan in this setting may help differentiate PRES from stroke. This is important in making treatment decisions, since mild to moderate hypertension may not be treated in stroke (permissive hypertension) but needs to be managed aggressively in PRES to prevent brain damage. Although a CT scan may show features consistent with PRES, FLAIR MRI is considered to be more sensitive for diagnosing PRES.1 The typical lesion seen on FLAIR MRI is bilaterally symmetric vasogenic edema affecting posterior regions of the brain. Most commonly the parietal and occipital lobes, brainstem, and cerebellum are affected. Classic MRI features of bilateral hyperintense parieto-occipital lesions on T2- or FLAIR-weighted images help in differentiating PRES from stroke.
Treatment includes optimum blood pressure control and treating the underlying cause if identified. Commonly used antihypertensive medications include labetolol, hydralazine, nitroglycerine, and calcium channel blockers such as nifedipine and amlodipine. Anticonvulsants should not be given for longer than 3 months without evidence of epileptogenic focus on EEG or without recurrent seizures. It is a reversible syndrome with excellent recovery in most patients within a few weeks. Early and accurate diagnosis helps ensure optimal outcomes.
Acknowledgments: The authors would like to thank Dr Barbara Koppel for her help with the diagnosis in this patient and with the treatment. Dr Koppel is an Attending in the Department of Neurology at New York Medical College and Metropolitan Hospital Center, New York.
References:
1. Alparslan M, Bora U, Hüseyin K, et al. Posterior reversible encephalopathy syndrome in a renal transplanted patient. Am J Case Rep. 2013;14:241-244.
2. Hinchey J, Chaves C, Appignani B, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med. 1996;334:494-500.
3. Casey SO, Sampaio RC, Michel E, Truwit CL. Posterior reversible encephalopathy syndrome: utility of fluid-attenuated inversion recovery MR imaging in the detection of cortical and subcortical lesions. AJNR Am J Neuroradiol. 2000;21:1199-1206.








 Conference / image credit ©Samon/stock.adobe.com Generated with AI")






