

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Re-Expansion Pulmonary Edema in an Older Woman
Re-expansion pulmonary edema is noncardiogenic and follows re-expansion of the lung after thoracentesis is performed for large amounts of pleural effusion or for pneumothorax.


Figure 1. (Click to enlarge all figures)



Figure 2.
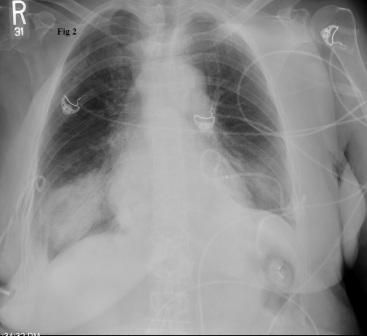


Figure 3.

A 73-year-old woman was admitted with a 1-week history of worsening shortness of breath and bleeding from a new left breast mass. She had a history of hypertension and type 2 diabetes mellitus. She was afebrile, hypertensive, tachycardic, and dyspneic on rest.
A breast examination showed an ulcerated and necrotic mass in the left breast that involved the nipple. There were multiple palpable, hard and fixed lymph nodes in the bilateral axillae and supraclavicular areas. There was dullness to percussion over both sides of the chest posteriorly, on the left greater than on the right. The rest of the physical examination findings were unremarkable.
Laboratory examination showed a normal complete blood cell count and the following: serum sodium, 112 mmol/L (normal range [NR], 136 to 145 mmol/L); serum potassium, 4.8 mmol/L (NR, 3.5-5.1 mmol/L); urea nitrogen, 13 mg/dL (NR, 7 to 18 mg/dL); creatinine, 0.5 mg/dL (NR, 0.6 to 1.3 mg/dL); serum osmolality, 240 mOsm/kg (NR, 285 to 295 mOsm/kg); urine osmolality, 891 mOsm/kg (NR, 50 to 1200 mOsm/kg); urine sodium, 63 mmol/L (NR, 20 to 110 mmol/L); thyroid-stimulating hormone, 3.2 µIU/mL (NR, 0.35-4.8 µIU/mL); cortisol, 19.5 µg/dL (NR, 6-21 µg/dL); and serum uric acid, 1.8 mg/dL (NR, 2.5 to 6.8 mg/dL).
A chest radiograph showed moderate to large bilateral pleural effusions (Figure 1). A biopsy of the patient’s breast mass was consistent with invasive ductal carcinoma, grade 3, estrogen receptor–negative/progesterone receptor–negative/human epidermal growth factor receptor 2–positive. Her metabolic parameters were consistent with a diagnosis of syndrome of inappropriate antidiuretic hormone secretion (SIADH).
The patient had bilateral pleural catheters placed to drain the large pleural effusions. She drained about 1.5 L of fluid from each side within a few hours after the procedure. Pleural fluid was exudative with negative cytology. A few hours later on the same day, her shortness of breath worsened. Oxygen saturation decreased to less than 90% on room air. However, the patient remained hemodynamically stable.
A new chest radiograph showed diffuse infiltrates over bilateral lower lung fields, consistent with re-expansion pulmonary edema (REPE) (Figure 2). Noninvasive ventilation with biphasic positive airway pressure (BIPAP) was started. The patient’s symptoms improved gradually over the next 24 hours. Serial chest radiographs showed significant resolution of the previously seen bilateral infiltrates (Figure 3). However, over the following weeks, recurrent bilateral pleural effusions developed for which pleurodesis was done.
Discussion
REPE is a type of noncardiogenic pulmonary edema that follows re-expansion of the lung after performing thoracentesis for large amounts of pleural effusion or pneumothorax. Symptomatic REPE, seen in fewer than 1% of cases, usually occurs within 1 or 2 hours after a thoracentesis.
Pathophysiologic mechanisms responsible for this phenomenon include the following:
-
Increased permeability of the pulmonary capillaries resulting from inflammation. Reperfusion of a previously collapsed lung coupled with ventilation leads to generation of free radicals and inflammatory mediators, such as interleukin-8, leukotriene B4, and monocyte chemotactic and activating factor. Another signaling pathway involving Rho (a small guanosine triphosphate–binding protein) and its target protein ROCK (Rho-associated coiled-coil–forming protein kinase) has been implicated. ROCK causes phosphorylation of myosin light chains, actomyosin contraction, and dysfunction of endothelial barrier cells-factors that contribute to increased permeability of the pulmonary capillaries.
- Increased pulmonary hydrostatic pressure caused by enhanced venous return.
- Altered lymphatic clearance.
- Decreased amounts of functional surfactant.1
Clinical features of REPE include chest discomfort, persistent cough (generally for greater than 20 min and irrespective of the presence of pinkish sputum), tachypnea, tachycardia, and worsening hypoxemia that may be refractory to oxygen therapy. The edema usually affects the entire re-expanded lung, but it may affect one lobe or the contralareral lung or it may be diffuse, affecting both lungs. Risk factors include age between 20 and 40 years, duration of collapse more than 72 hours, and rapid lung expansion after drainage of large volumes of pleural fluid (more than 1.5 L).1
Diagnosis usually is based on the characteristic serial radiographic features. CT findings include patchy areas of ground-glass opacity frequently combined with consolidation and interlobular and intralobular interstitial thickening, suggesting mixed permeability and hydrostatic edema as the underlying pathogenic mechanism.2 The infiltrates usually occur peripherally and in gravity-dependent areas. Most commonly they occur unilaterally but contralateral cases have also been described.
Continued on next page.
Treatment
Treatment of patients with REPE varies from oxygen supplementation for mild cases to noninvasive ventilation for moderate cases to intubation and invasive ventilation for severe cases. In patients who require invasive ventilation, symptoms usually improve within 24 to 48 hours. In unilateral cases, lying on the unaffected side may be therapeutic.
Most patients recover completely within a week. In rare cases, however, patients may sequester large amounts of fluid in the lungs, which may lead to shock and death.
Preventive strategies include using low negative pressure (less than negative [Ë] 20 cm H2O) for suction during tube thoracostomy and limiting drainage of pleural fluid to 1 to 1.5 L.1 However, recent studies have shown that large effusions can be drained completely as long as chest discomfort or end-expiratory pleural pressure less than Ë20 cm H2O does not develop.3 For this reason, pleural manometry is being used increasingly for draining large pleural effusions.
Chest discomfort experienced by patients during thoracentesis may indicate a significant drop in pleural pressures. In such cases, thoracentesis should be stopped.
Role of imaging
This patient’s case highlights the importance of prompt recognition of REPE and early treatment with BIPAP, which may obviate the need for intubation. Imaging plays a vital role in its early recognition. Chest radiographic features may include unilateral airspace opacification of the re-expanded lung. High-resolution chest CT further aids in differentiating REPE from other conditions such as aspiration pneumonia and pleural effusion.
The CT findings that have been described most commonly include ipsilateral ground-glass opacities, smooth septal thickening, consolidation and persistent foci of atelectasis. Less common features include air bronchograms and nodules. These findings in combination with the clinical features mentioned above should make the clinician suspect this condition and treat it appropriately with either noninvasive or invasive mechanical ventilation.
References:
1. Kasmani R, Irani F, Okoli K, Mahajan V. Re-expansion pulmonary edema following thoracentesis. CMAJ. 2010;182:2000-2002.
2. Baik JH, Ahn MI, Park YH, Park SH. High-resolution CT findings of re-expansion pulmonary edema. Korean J Radiol. 2010;11:164-168.
3. Feller-Kopman D, Berkowitz D, Boiselle P, Ernst A. Large-volume thoracentesis and the risk of reexpansion pulmonary edema. Ann Thorac Surg. 2007;84:1656-1661.












