

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Paroxysmal Supraventricular Tachycardia: Diagnosis and Management
Management options for PSVT in a stable patient include vagal maneuvers, medications, and electrical synchronized cardioversion.


Figure 1. ECG monitor (Click figures to enlarge)
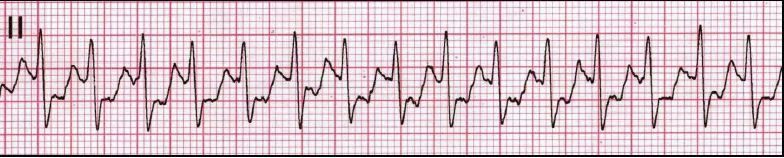


Figure 2. 12-lead ECG
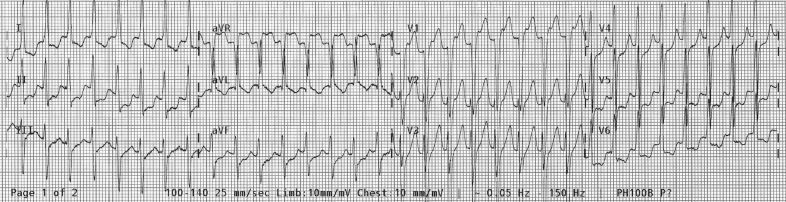


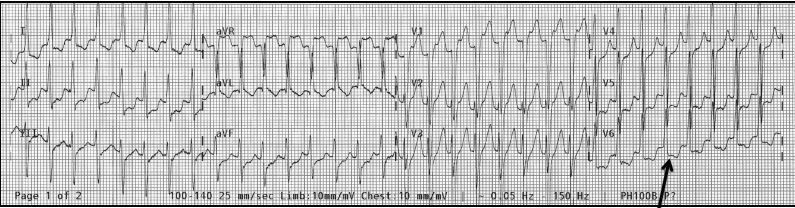
Figure 3. Retrograde P wave seen at arrow in lead V6.
A 27-year-old woman without significant medical history presented to the emergency department (ED) with palpitations. She said she had noted the sensation of a rapid heartbeat during the past 30 minutes. She denied syncope, dizziness, weakness, chest pain, dyspnea, or other significant complaints.
On examination, she was alert and oriented, in no apparent distress. Vital signs were significant for blood pressure, 119/71 mm Hg; pulse, approximately 180 beats/min; respiratory rate, 20 breaths/min; temperature, 36.2°C (97°F); and oxygen saturation, 98% on room air. The ECG monitor demonstrated the rhythm strip in Figure 1. Cardiac examination found an extremely rapid, regular rhythm. The remainder of the examination was normal. A 12-lead ECG was performed; results are seen in Figure 2.
Based on the clinical information noted in this case, including the ECGs in Figures 1 and 2, the most appropriate management is:
A. Amiodarone 150 mg IV over 15 minutes.
B. Adenosine 6 mg IV push.
C. Procainamide 17 mg/kg IV over 45 minutes.
D. Electrical cardioversion at 50 joules.
Answer: B. Adenosine 6 mg IV push.
Discussion
The differential diagnosis of a regular narrow QRS complex tachycardia includes sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT), atrioventricular reciprocating tachycardia of Wolff-Parkinson-White syndrome, atrial flutter, and atrial tachycardia (see Table). PSVT is the second most frequently encountered dysrhythmia of this group. PSVT is seen in patients of all ages and both sexes; it is more common in younger woman for unknown reasons. The dysrhythmia is most often found in otherwise healthy patients without significant underlying heart disease. The focus of the dysrhythmia is most often in the atrioventricular node; in a minority of cases, the focus is located in atrial tissues.
PSVT is a regular narrow QRS complex tachycardia (Figure 3). The QRS complex is of normal width, usually less than 0.08-0.10 seconds in duration. PSVT is rapid and regular. In the adult patient, the rate is usually 170 to 180 beats/min with a range of 130 to 240 beats/min. P waves are usually not seen. Since atrial and ventricular depolarizations usually occur near-simultaneously, the P waves are frequently buried in the QRS complex and are totally obscured; in a minority of presentations, a P wave is noted-the so-called retrograde P wave (Figure 3, arrow)-and can be found either before, during, or after the QRS complex. Lastly, in certain patients, widespread ST-segment depression is seen; most often, this finding is only related to the rapid rate, the so-called rate-related ST-segment depression. Of course, in a patient with clinically correlated, concerning symptomatology after conversion, attention should be paid to the ST-segment change.
Management options include vagal maneuvers, medications, and electrical synchronized cardioversion. Medication options include the following: adenosine (6 mg followed by 12 mg IV push); beta-adrenergic blocking agents (metoprolol 5 mg IV over several minutes); calcium channel antagonists (diltiazem 0.25 mg/kg IV over 10 to 15 minutes); sodium channel antagonists (procainamide 17 mg/kg IV over 45 minutes); amiodarone (150 mg IV over 10 to 15 minutes). Synchronized electrical cardioversion can start at 50 joules (J) as initial energy level and escalate as necessary. Management is dependent on the hemodynamic status of the patient. In the unstable patient, PSVT is usually appropriately and easily managed with a trial of adenosine using the higher dose of 12 mg IV; if unsuccessful, synchronized electrical cardioversion starting at 50 J with sedation-if the clinical situation allows-is usually curative. In a hemodynamically stable patient, vagal maneuvers followed by adenosine are usually effective. If unsuccessful, the other agents listed above can be employed.
Case Conclusion
The ECGs in Figures 1 and 2 were felt to demonstrate PSVT. The patient was stable on presentation and vagal maneuvers were attempted initially but were unsuccessful. The patient then received adenosine 6 mg IV. She was immediately converted to sinus tachycardia at a rate of 110 beats/min; a repeated 12-lead ECG was entirely normal, other than the rate. She remained stable without recurrence of dysrhythmia for 2 hours in the ED; she was discharged with recommendations to follow-up with a cardiologist as an outpatient.
Take-Home Points
1. The differential diagnosis of a regular narrow QRS complex tachycardia includes paroxysmal supraventricular tachycardia, sinus tachycardia, atrial flutter, and atrial tachycardia.
2. AVN blocking agents, including vagal maneuvers, adenosine, beta-adrenergic blockers, and calcium antagonists, are most often appropriate for PSVT in a stable patient. Vagal maneuvers and intravenous adenosine are the preferred therapies in most instances.
3. For the unstable patient with PSVT, a trial of adenosine at 12 mg IV is appropriate; if unsuccessful, adenosine is followed by synchronized electrical cardioversion, with sedation if the clinical situations allows.
Table. Differential Diagnosis of Narrow Complex Tachycardia
Atrial fibrillation
WPW, Wolff-Parkinson-White sydrome.













