

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Mycosis Fungoides as Cause of Erythroderma
The patient was treated with a combination of topical corticosteroids, oral retinoids, and psoralen with ultraviolet A (PUVA) therapy, with significant improvement in his symptoms over time.


Figure 1. (Click all images to enlarge.)


Figure 2.


Figure 3.


Figure 4.



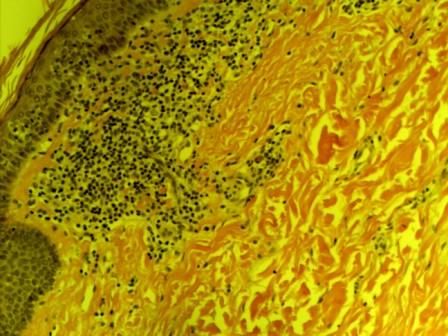
Figure 5. H&E stain 100X.
A 60-year-old man was seen in dermatology for large confluent, hyperpigmented, erythematous, pruritic patches and plaques involving more than 90% of his body surface area (BSA) (Figures 1-4). There was no lymphadenopathy or hepatosplenomegaly. His medical history was notable for hypertension, diabetes mellitus, and seizure disorder. His medications included losartan, aspirin, rosuvastatin, and phenytoin.
Skin biopsy showed lymphocytic infiltrate involving the epidermis and dermis without spongiotic microvesiculation. Characteristic “haloed cells” were seen (Figure 5). Peripheral blood flow cytometry was negative for clonal disease (ie, T-cell gene rearrangement). Bone marrow biopsy was unremarkable. Pan CT did not reveal any abnormalities.
Which of the following do you believe is the cause of his erythroderma? What led you to this impression?
A. Plaque psoriasis
B. Mycosis fungoides/Sezary syndrome
C. Atopic dermatitis
D. Drug hypersensitivity reaction
E. Something else entirely
Answer: B. Mycosis fungoides
This patient’s clinical and histologic findings were consistent with mycosis fungoides (MF) without Sezary syndrome. He was treated with a combination of topical corticosteroids, oral retinoids, and psoralen with ultraviolet A (PUVA) therapy, with significant improvement in his symptoms. At the time of diagnosis, the patient was in stage IIIA (T4N0M0B0) as per the TNMB staging system. His symptoms slowly began to improve after the initial 6 months of treatment and continued to improve over the next 1.5 years. His condition was downgraded to stage 1B (T2N0M0B0) after 2 years. His current medications include a maintenance dose of the second-generation retinoid acitretin (25 mg daily); triamcinolone 0.1% ointment applied twice daily to the affected areas; and hydroxyzine 50 mg daily for itching. Median survival of patients with stage III disease is 4 to 6 years as compared with stage IB for which the median survival exceeds 11 years.
Discussion
Erythroderma refers to the presence of diffuse erythema that involves more than 90% of BSA. Its diagnosis is easy, but determination of its cause is more difficult. Differential diagnoses include plaque psoriasis, atopic dermatitis, drug hypersensitivity reactions, and rarely mycosis fungoides/Sezary syndrome (MF/SS). Clues that aid in determining the correct diagnosis include mode of onset, preceding drug history (eg, penicillins, sulfa drugs, phenytoin, allopurinol can lead to drug reaction with eosinophilia and systemic symptoms-DRESS syndrome), organ involvement, and presence of prior inflammatory dermatoses. The absence of any of the foregoing in our patient suggested a secondary etiology.
Mycosis fungoides and Sezary syndrome are the most common types of cutaneous T-cell lymphomas (CTCL). MF is a mature T-cell non-Hodgkin lymphoma most commonly localized to the skin. It can, however, be aggressive and spread to lymph nodes, blood, and other organs, such as the liver, spleen, and gastrointestinal tract. Sezary syndrome refers to erythrodermic CTCL with blood involvement. Diagnostic criteria for Sezary syndrome include1: absolute Sezary cell count of at least 1000 cells/µL, and CD4/CD8 ratio of >10 or T-cell clonality by peripheral blood flow cytometry.
The etiology of MF is uncertain. Occupational exposure to solvents and HTLV-1 have been implicated. The annual incidence of MF is about 6 cases/million and accounts for 4% of all non-Hodgkin lymphomas.2 It usually affects adults 55 to 60 years of age with a 2:1 male to female ratio. It is more common in blacks.
Presentation
Clinical features of MF include presence of progressive skin lesions such as patches, plaques, papules, tumor, erythroderma, and hypopigmented or hyperpigmented lesions in non–sun-exposed locations. Patients may have associated alopecia. Extracutaneous manifestations with involvement of lymph nodes and other organs usually occur with extensive skin involvement. The lesions are very pruritic and may cause patients significant distress. The underlying immune dysfunction may lead to opportunistic infections and occurrence of secondary malignancies, particularly lymphomas.
Clinicians should have a high index of suspicion for MF especially while evaluating patients with erythroderma and chronic nonspecific dermatitis that has been resistant to standard treatment. Skin biopsy is the standard tool for making a diagnosis. Multiple skin biopsies are preferable. The skin lesions with the most induration should be selected and a minimum 4-mm punch biopsy should be performed. The International Society for Cutaneous Lymphoma and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer3 have proposed a point-based scoring system for early diagnosis and staging of MF.3 This is based on clinical, histopathologic, molecular biologic, and immunopathologic parameters.
Clinical parameters include persistent or progressive patches and plaques affecting non–sun-exposed areas; histologic parameters include presence of superficial lymphoid infiltrate, epidermotropism without spongiosis and lymphoid atypia; molecular parameters include detection of clonal TCR gene rearrangement; and immunologic parameters include <50% CD2+, CD3+ and CD5+ cells, <10% CD7+ cells, and epidermal/dermal discordance of CD2, CD3, CD5, or CD7.4
For treatment of early-stage disease, skin-directed therapies are preferred over systemic therapies. Skin-directed therapies include topical corticosteroids, retinoids, nitrogen mustard, psoralen enhanced ultraviolet A light (PUVA) therapy, and total body electron beam radiation. Systemic therapy for advanced disease includes oral retinoids, IFN-alpha, alemtuzumab (monoclonal antibody), chemotherapy (methotrexate, doxorubicin), and histone deacetylase inhibitors such as romidepsin and vorinostat.
Outcome
The main predictor of outcome in MF is the overall stage. Limited skin disease is a good prognostic factor. A range of other factors, however, including male sex; older age (>60 years); folliculotropic variant plaques; large-cell transformation; and nodal, visceral, or blood involvement portend a poor prognosis based on the Cutaneous Lymphoma International Prognostic index.5
Although stage IIIA was the initial diagnosis in our patient, he was successfully treated with combination therapy and his condition was downgraded to stage IB. The median survival of patients with stage IB is greater than 11 years. At this time, his prognosis seems favorable. He is being monitored regularly for development of progressive disease and Sezary syndrome.
References:
1. Vonderheid EC, Bernengo MG, Burg G, et al. Update on erythrodermic cutaneous T-cell lymphoma: report of the International Society for Cutaneous Lymphomas. J Am AcadDermatol. 2002;46:95-106.
2. Criscione VD, Weinstock MA. Incidence of cutaneous T-cell lymphoma in the United States, 1973-2002. Arch Dermatol. 2007;143:854-859.
3. Olsen E, Vonderheid E, Pimpinelli N, et al. Revisions to the staging and classification of mycosis fungoides and Sezary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC).Blood. 2007;110:1713-1722.
4. Pimpinelli N, Olsen EA, Santucci M, et al. Defining early mycosis fungoides. J Am Acad Dermatol. 2005;53:1053-1063.
5. Benton EC, Crichton S, Talpur R, et al. A cutaneous lymphoma international prognostic index (CLIPi) for mycosis fungoides and Sezary syndrome. Eur J Cancer. 2013;49:2859-2868.







