

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Maxillary Pain of One Year’s Duration in a Young Man: Complex odontoma? Regional odontodysplasia? Amelogenesis imperfecta?
A 16-year-old boy was complaining of pain in the maxillary left incisor/cuspid region. He had been experiencing discomfort for 1 year. He was otherwise healthy and a review of his other systems was unremarkable.
Patient Presentation
A 16-year-old boy was complaining of pain in the maxillary left incisor/cuspid region. He had been experiencing discomfort for 1 year.
Medical History
The patient was otherwise healthy. He had no medical problems. A review of his other systems was unremarkable.
Clinical Findings
Examination showed that the patient lacked the maxillary left incisors and cuspid tooth. There was a raised area of approximately 1.5 cm in the area where the teeth should have been located (Figure 1). The tissue was of normal color and was firm to the touch.



Figure 1
.
Laboratory Findings
The patient presented without laboratory findings and none were requested based on the examination findings. Imaging, detailed below, suggested a benign tooth-like structure in the region of the swelling.
Radiographic Findings
Radiographic imaging of the region (Figure 2) revealed malformed and impacted teeth, presumably the maxillary central, lateral incisor, and cuspid. The pulp chambers were large and root canals wide. The root portion of the structures was shortened and poorly outlined. Hypoplastic dentin and thin poorly mineralized enamel were barely evident. Remnants of follicular tissue surrounded the teeth below the lateral incisor. The cuspid was radiolucent with a "moth eaten" appearance.


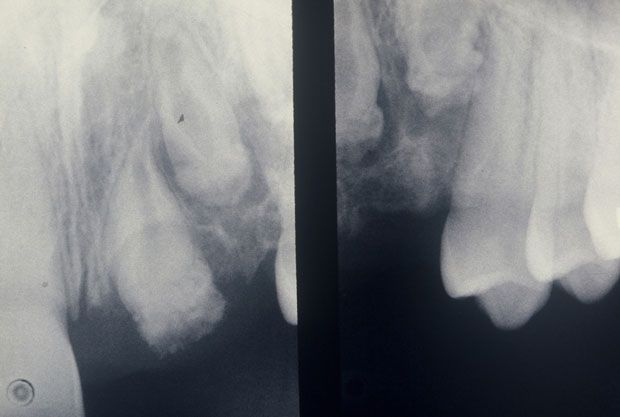
Figure 2.
Biopsy Results
Given the clinical and imaging findings an excisional biopsy was performed. Sections of soft tissue revealed irregular segments of mildly cellular fibrous connective tissue. Focal cellular concentrations contained eosinophilic, amphophilic, and basophilic calcifications. Scattered throughout the tissue were nests of dormant-appearing odontogenic epithelium (Figure 3, left; on next page), some of which were clear cells.


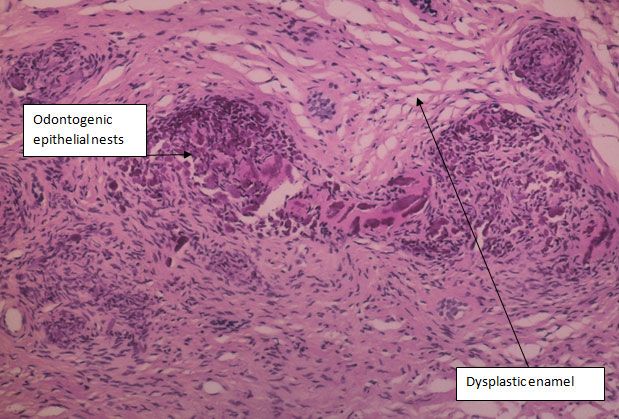

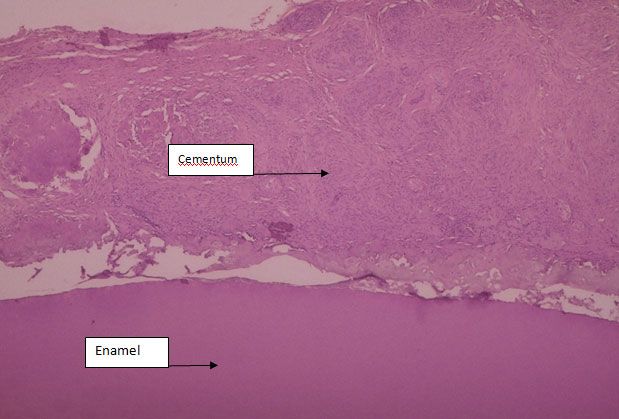
Figure 3.
The radicular portion of the biopsied tissue is coated with a layer of cellular cementum of variable thickness (Figure 3, right) with an adjacent layer of fibrous connective tissue. The coronal portion is covered by a thin layer of dysplastic enamel. The structures removed at biopsy are depicted in Figure 4.



Figure 4.
Photograph showing the tooth-like structures removed at biopsy
Differential Diagnosis
Given the above findings, the following were considered as possible diagnoses:
• Compound odontoma
• Complex odontoma
• Regional odontodysplasia
• Dentinogenesis imperfecta
• Amelogenesis imperfecta
Final Diagnosis
The clinical findings, radiographic presentation, and histology supported the diagnosis of regional odontodysplasia (RO). In patients with regional odontodysplasia, adjacent erupted teeth are normal. The radiographic appearance of the unerupted structure(s) is of malformed teeth with thin radio-opaque contours. It is difficult to distinguish the enamel from the dentin and there are wide open pulp chambers, which give the structure(s) a characteristic ‘ghost-like' appearance.
Dentinogenesis and amelogenesis imperfecta were both ruled out because these conditions involve the entire dentition. Complex and compound odontomas tend to involve more defined structures with well formed borders. There is often a surrounding soft tissue capsule.


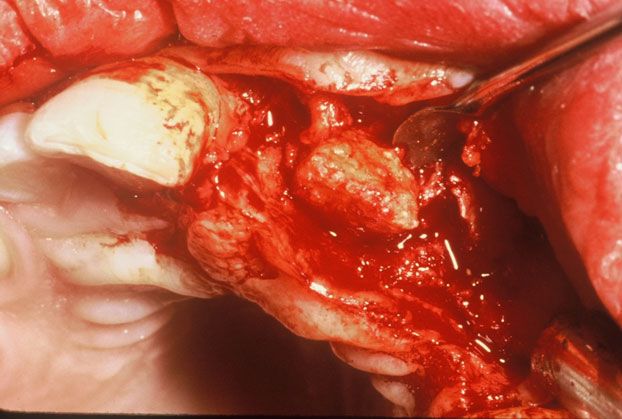
Figure 5.
Management
The patient's problem was treated with complete surgical excision of the tooth-like structures (Figure 5). The post-treatment course was uneventful and no additional treatment was provided. Follow-up dental reconstruction was to be considered.
Discussion
RO is a rare, benign non-hereditary condition that is characterized by abnormal development of the dental hard tissues. The condition is more common in women but there is no racial predilection. It can affect both primary and permanent teeth and occurs most typically in the maxilla although cases have been reported in the mandible. The cause is unknown but local trauma as well as radiation exposure, hypophosphatasia, hypocalcemia, and hyperpyrexia have been implicated.
In the primary dentition, teeth may erupt but be malformed and hypocalcified with brown discoloration. In adult or permanent dentition, these structures usually are not erupted. Adjacent permanent teeth erupt normally. Lesions are typically localized to one area, but can occur in multiple regions.
The condition does not typically cause pain, but there can be associated soft tissue swelling and fibrous enlargement with partial eruption. Both mesodermal and ectodermal tissues are involved in the development of the structures.
Treatment is somewhat controversial. Some clinicians recommend leaving the structures in place to preserve the alveolar bone, while others recommend surgical removal. Grafting and implant strategies make alveolar reconstruction and tooth replacement very reasonable following surgery.
Teaching Points:
1. Delayed eruption coupled with swelling in a localized region of the maxilla or mandible of a young female can indicate the presence of a regional odontodysplasia or compound or complex odontoma.
2. Examination should include assessment via panoramic imaging.
3. Treatment is excisional biopsy. Surgery should be performed after puberty and the full development of the mandible or maxilla. This timing will improve the aesthetic outcome of post-surgical dental reconstruction.
References:
Bibliography
1. Gǜndǜz K, Zengin Z, Celenk P, et al. Regional odontodysplasia of the deciduous and permanent teeth associated with eruption disorders: a case report. Med Oral Patol Oral Cir Bucal. 2008;13:E563-566.
2. Magalhães AC, Pessan JP, Cunha RF, Delbem AC. Regional odontodysplasia: case report. J Appl Oral Sci. 2007; 15:465-469.
3. Thimma Reddy BV, Vinay Reddy KK, Sunil B, et al. Regional odontodysplasia. J Indian Soc Pedod Prev Dent. 2010; 28:315-318.
4. Cabral L A G, Carvalho YR, Moraes E, et al. Regional odontodysplasia: a report of 3 cases. Quintessence Int.1994;25:141â145.
5. McCall J O, Wall S S. Clinical dental roentgenology. 3rd ed. Philadelphia: W B Saunders, 1952.
6. Zegarelli E V, et al. Odontodysplasia. Oral Surg Oral Med Oral Pathol. 1963;16:187â193.
7. Gumurii O Z, et al. Regional Odontodysplasia.
J Nihon Univ Sch Dent.
1993;35:209â212.
8. Neupert E A, Wright J M. Regional odontodysplasia presenting as a soft tissue swelling. Oral Surg. 1989;67:193â196.
9. Sabah E, Eden E, Unal T. Odontodysplasia: report of a case. J Clin Ped Dent. 1992;16: 115â118.
10. Crawford PJ, Aldred MJ. Regional odontodysplasia: a bibliography. J Oral Pathol Med. 1989;18:251-63.









Obesity Linked to Faster Alzheimer Disease Progression in Longitudinal Blood Biomarker Analysis
December 2nd 2025Biomarker trajectories over 5 years in study participants with AD show steeper rises in pTau217, NfL, and amyloid burden among those with obesity, highlighting risk factor relevance.


