

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Face to Face With Skin Conditions: A Photo Quiz
Meet patients’ facial skin problems head-on by gaining a familiarity with the common problems and symptoms. This week’s photo quiz offers a variety of presentations to test your prima facie knowledge.



Question 1:
A 48-year-old man presented for treatment of herpes zoster. As an incidental finding, numerous flesh-colored, asymptomatic papules were noted on the central face. They have no malignant potential and no serious systemic associations. The disorder is autosomal dominant.
NEXT QUESTION »
For the discussion, click here.


Question 2:
This man’s skin condition appears as erythematous plaques or patches topped by white or yellow scale. It most often affects the scalp and the face, particularly the ears, eyebrows, and nasal alae. In persons of color, it may appear simply as white, minimally scaly patches on the face underlying the eyebrows. It can become secondarily infected with gram-positive organisms. The man has seborrheic dermatitis.
NEXT QUESTION »
For the discussion, click here.



Question 3:
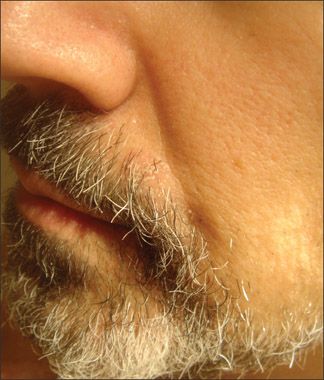
A close-up view of a patient with rosacea shows striking hypertrophy of the nasal soft tissue. Adjacent portions of cheeks show extensive papule formation and surface irregularity from overgrowth of sebaceous tissue and connective tissue. A tiny venous lake is seen on the left lower lip.
NEXT QUESTION »
For the discussion, click here.
For the answer, click here.



Question 4:
A 9-year-old girl is brought by her mother because of the acute onset of a facial rash. There is no associated itching, and the child is, and has been, otherwise healthy. The linear arrangement of 1 or more parallel bands composed of 2- to 4-mm flat-topped papules on the face or on an extremity is classic for an idiopathic, asymptomatic eruption that favors children.
NEXT QUESTION »
For the discussion, click here.



Question 5:
A 77-year-old man sought medical attention because of a painful group of “sores” near his mouth. He was just recovering from community-acquired pneumonia. The attack was precipitated by the temporarily impaired immune response associated with his pulmonary infection. The clustered grouping included small, shallow erosions surmounting a slightly indurated plaque.
NEXT QUESTION »
For the discussion, click here.



Question 6:
A 7-year-old boy presented with a solitary, nearly circular, very pruritic inflammatory facial lesion. Annular lesions suggest dermatophytosis. The intensity of the inflammatory response suggests a nonhuman source for the fungus (the presence of which was verified by potassium hydroxide).
NEXT QUESTION »
For the discussion, click here.



Question 7:
Despite curettage several months earlier, the facial rash on this 4-year-old boy had spread across both cheeks and was now mildly pruritic. Note the discrete, smooth, pearly or flesh-colored, dome-shaped papules with central umbilication.
NEXT QUESTION »
For the discussion, click here.



Question 8:
A 5-year-old boy was brought to the ED because of a rash that covered his entire body. It had started 2 days earlier, initially on his face, abdomen, and legs, and had spread to his back, buttocks, and hands. He had a 1-day history of tactile fever. He had no sick contacts and no significant medical history. He appeared to be nontoxic; he was afebrile and his vital signs were stable. His skin had patches of erythema and exfoliation that were slightly tender to palpation and felt warm to the touch.
ANSWER KEY »
For the discussion, click here.
ANSWER KEY:
Question 1. A
Question 2. E
Question 3. A
Question 4. C
Question 5. B
Question 6. B
Question 7. B
Question 8. D





Atopic Dermatitis: The Pipeline and Clinical Approaches That Could Transform the Standard of Care
September 24th 2025Patient Care tapped the rich trove of research and expert perspectives from the Revolutionizing Atopic Dermatitis 2025 conference to create a snapshot of the AD care of the future.


