

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Benign Lymphoepithelial Cysts Associated With HIV Infection


Figure 1. Ultrasound R and L neck. (Click to enlarge)
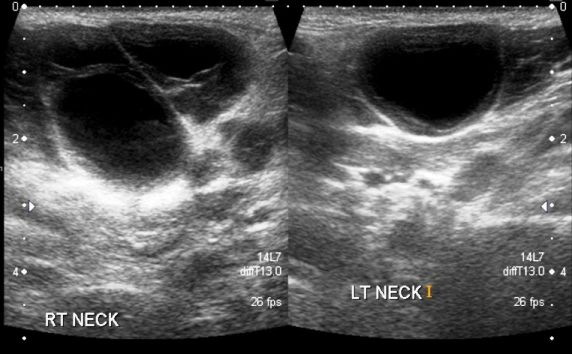


Figure 2. Transverse L neck.
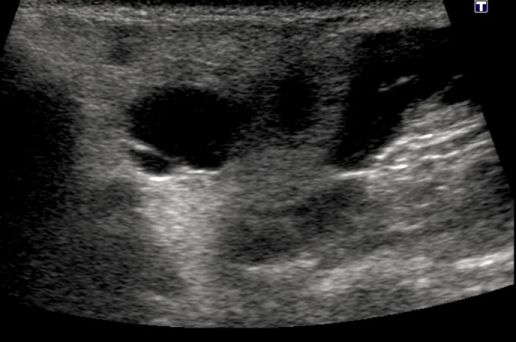


Figure 3. Transverse R neck.

A 40-year-old African American man presented to an urban emergency department with a 1-year history of bilateral painless swelling in his neck. He denied fever, dysphagia, dysphonia, paresthesias, sore throat, congestion, cough, wheeze, or shortness of breath.
The patient had incurred a jaw fracture 3 years earlier, which required inter-maxillary fixation to repair. His medical, surgical, and family histories were otherwise unremarkable. He denied any intravenous drug use and admitted to heavy alcohol and tobacco use. He was sexually active at the time of presentation with one female partner.
On physical examination, the patient was normotensive and afebrile. There were no skin color changes or indurations surrounding the swelling. On palpation, the swelling was non-tender, soft, and mobile but did not feel fluid-filled.
Ultrasound of the neck was ordered to determine the composition of the swelling. Findings included bilateral parotid masses identified as enlarged parotid glands with multiple 2- to 3-cm cysts present within the glandular tissue (Figures 1-3).
What diagnosis do the ultrasound images suggest to you?
Answer: The ultrasound findings were consistent with a diagnosis of benign lymphoepithelial cysts, an HIV-associated infection. The patient was tested for HIV on site and found to be positive.
Discussion
Parotid gland enlargement affects up to 10% of adults with HIV/AIDS.1-3 Benign lymphoepithelial cysts are the most common salivary gland pathology associated with HIV, and they are an easily recognized feature of HIV within populations aware of the disease.4
Benign lymphoepithelial cysts are characterized by painless, fluctuant, bilateral parotid swelling associated with cervical lymphadenopathy.1,4 Cysts can be firm or soft, depending on the degree of lymphoproliferative infiltration. The impetus for presentation-as with our patient-is often cosmetic because of the large and deforming nature of the cysts.2
In the case presented here, diagnosis was made via ultrasound. Ultrasound is uniquely suited to imaging these kinds of cystic and lymphoproliferative masses because it is simple, painless, noninvasive, and without radiation.3 Typically, the parotid gland is an echogenically homogenous structure surrounded by less echogenic muscle and fat.3 Findings indicative of lymphoepithelial cysts, however, are large, well-circumscribed hypoechogenic areas with occasional septa as demonstrated by the ultrasound images in Figures 1, 2, & 3.
Treatment of benign lymphoepithelial cysts is controversial. While some sources state that the only indication for treatment is cosmetic,4 others argue that the interstitial lymphoid proliferation in the parotid gland should be considered a precursor for the development of malignancy.2
Current treatment options include antiretroviral therapy, repeated drainage, radiation, sclerotherapy, and surgery. Antiretroviral therapy is the standard of care for HIV infection and thus a very reasonable first-line therapy.4 Unfortunately, most cysts do not completely regress with antiretroviral therapy alone. Drainage of cysts is popular but ultimately ineffectual because cysts recur in a matter of months.1,4 Radiation therapy, a far more expensive option, also does not appear to confer any long-term control.4
Currently, the most successful options for complete regression of cysts appear to be sclerotherapy and surgery.4,5
Treatment
After having a positive HIV test in the ED setting, the patient was counseled by a patient navigator. He was scheduled to see an infectious disease specialist affiliated with the hospital within the week. On confirming his HIV status with Western blot, further labs were ordered, including CD4 cell count, HIV-RNA, and PhenoSense Comprehensive. The results of the patient’s labs will assist in making a decision whether or not to start antiretroviral therapy, and the patient can be further counseled regarding available options for reducing the benign lymphoepithelial cysts.
Conclusion
The patient presented in an ED setting with no symptoms other than the bilateral swelling in his neck. The differential diagnosis for such masses was broad and included lymphoma, Sjögren syndrome, and malignancy.3 The gradual presentation and absence of concurrent symptoms, however, made the other possible diagnoses less likely. By utilizing ultrasound to better characterize the masses, we were able to arrive quickly at a diagnosis and avoid more invasive measures.
While the initial presentation of HIV is not typically associated with isolated bilateral neck masses, it is not so uncommon that HIV should not continue to be part of the primary care provider’s differential diagnosis. Basic working knowledge of this diagnosis and its sonographic features may aid the primary care provider in appropriately testing patients for HIV and promptly beginning treatment when necessary.
References:
1. Shanti RM, Aziz SR. HIV-associated salivary gland disease. Oral Maxillofacial Surg Clin N Am. 2009;21:339-343.
2. Mandel L, Surattanont F. Regression of HIV parotid swellings after antiviral therapy: case reports with computed tomographic scan evidence. Oral Med Oral Pathol Oral Radiol Endod. 2002;94:454-459.
3. Mandel L. Ultrasound findings in HIV-positive patients with parotid gland swellings. J Oral Maxillofac Surg. 2001;59:283-286.
4. Steehler MK, Steehler MW, Davison SP. Benigh lymphoepithelial cysts of the parotid: long-term surgical results. HIV/AIDS-Research and Palliative Care. 2012;4:81-86.
5. Berg EE, Moore CE. Office-based sclerotherapy for benign parotid lymphoepithelial cysts in HIV-positive patient. Laryngscope. 2009;119:868-870.





Common Side Effects of Antiretroviral Therapy in HIV Infection
February 7th 2013What are some of the more common side effects of antiretroviral therapy, and what can the primary care physician do to help manage these effects? In this podcast, infectious disease expert Rodger MacArthur, MD, offers insights and points readers to updated comprehensive guidelines.



