

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Red Herring Urinalysis
A 38-year-old woman has had abdominal pain x4 days that worsens on hip flexion. Imaging, labs are inconclusive. But there was that urine culture ...


Figure 1. (Please click to enlarge)
History: A 38-year-old woman presents to the emergency department complaining of 4 days of abdominal pain. She says the pain was initially generalized, but a day or two later localized to the right midabdomen, with occasional radiation to her low back and right hip. At that time she went to another hospital where she underwent a CT scan and abdominal ultrasound and lab work was performed. All results were normal except for evidence of a kidney infection for which she has been taking Cipro for the past 2-3 days.
Her pain has persisted. It has neither improved nor worsened. She states the pain is worse with walking or flexing her hip. She denies any current or recent fever, chills, dysuria, vaginal discharge, diarrhea or vomiting but says she has been nauseated.
She denies any significant chronic medical history, but has had a kidney infection in the past, many years ago, which she states felt similar, but not identical. She does not smoke tobacco or use illicit drugs. Her last sexual activity was about a month ago with a new partner, but they used condoms.
You are able to obtain the records from the other hospital and discover that the urinalysis had >10 epithelial cells/HPF, and the urine culture was non-diagnostic. Of course no one ever contacted her about this because a negative urine culture did not trigger an inbox message.
Examination: The patient’s vital signs were normal including an oral temperature. Results of the physical examination were normal except for mild right-sided abdominal tenderness, which was located more in the lower- and mid-abdomen than in the upper abdomen. There was no CVA tenderness and a pelvic exam was unremarkable without cervical tenderness.
Initial concerns:• Resistant pyelonephritis
• Pelvic inflammatory disease
• Masked appendicitis
• Ovarian cyst
• Biliary colic
Laboratory results: WBC 6.7 with 75% PMNs, beta-HCG negative, UA negative
Next steps
1. What other physical examination should be performed?
2. What other laboratory testing should be considered?
3. What if any additional or repeat imaging should be considered?
Please click below for answers and discussion.
Answers1. What other physical examination should be performed? Obturator sign and psoas sign help pick up retrocecal appendicitis, which is the most commonly missed type of appendicitis because exam findings can be unimpressive and CT may be falsely negative. Both obturator and psoas signs were positive.
2. What other laboratory testing should be considered? When the WBC is normal but you are still concerned about appendicitis, add an ESR and/or a CRP as they tend to be more sensitive than a WBC count. The ESR was elevated at 23 mm/h. It was hypothesized that inflammatory markers probably would have been higher had the patient not been on antibiotics.
3. What if any additional or repeat imaging should be considered? A pelvic ultrasound is warranted if you are worried about an ovarian condition and a repeat CT if you are worried about appendicitis. CT scan showed RLQ inflammation just anterior to the psoas muscle, but the appendix was not identified. Partially treated appendicitis was suspected, but since the diagnosis was not definitive the decision was made to admit to the surgical service for serial abdominal exams off all medication.
Discussion
Appendicitis is one of the most common surgical emergencies. Like most medical conditions, only a minority of cases present classically, many cases present with mostly typical features, and a significant minority present atypically, often fooling the clinician. Historical atypia can include symptom duration greater than 3 days, ectopic pain location, urinary symptoms, and diarrhea.
The physical exam can also be atypical. Retrocecal appendicitis is infamous for being missed because of an unimpressive abdominal exam, especially when the obturator and psoas signs are not checked. These examination maneuvers are not necessary when there is obvious RLQ tenderness, but should always be checked when there is right-sided abdominal pain without significant tenderness.
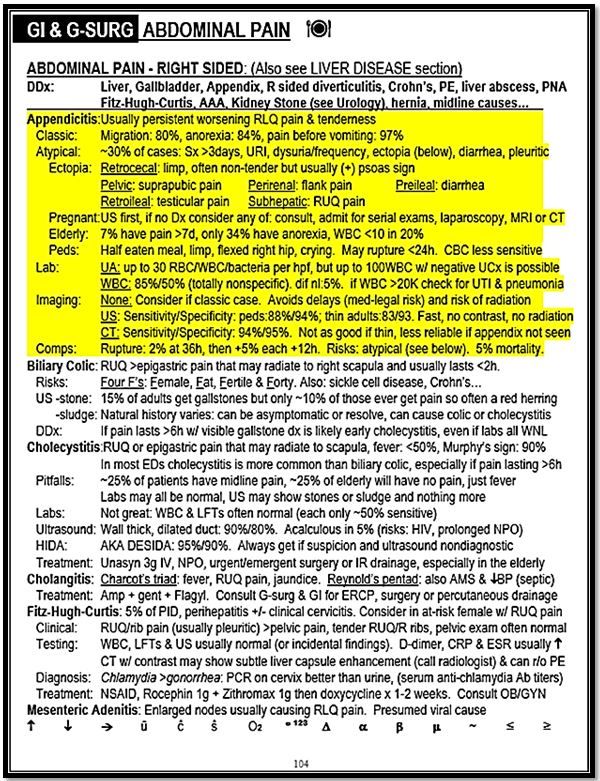
Diagnostic testing can also lead even seasoned physicians astray. Urinalysis can show pyuria, even in a catheterized specimen. Bacteria, however, are usually not present. In addition the blood WBC count is normal in about 15% of cases of confirmed appendicitis. CT scan is very sensitive, but like most tests in medicine, also is not perfect. (Click on image in Figure 1 at right for more information and to enlarge.)
In this case the original urinalysis result was a red herring that led to the patient being started on antibiotics, which likely slowed progression of the appendicitis to a smolder, made follow up testing less reliable (masking), and contributed to a delay in diagnosis and complications, as in this case.
Case conclusion: The patient was admitted for observation and antibiotics were held. The following afternoon due to lack of improvement and a rise in inflammatory markers she was taken to the OR where retrocecal appendicitis was diagnosed. The appendix was noted to be significantly inflamed and adherent to the cecum. The case was converted from laparoscopic to open when she suffered a colonic perforation when the appendix was dissected off of the cecum.


