

- Clinical Technology
- Adult Immunization
- Hepatology
- Pediatric Immunization
- Screening
- Psychiatry
- Allergy
- Women's Health
- Cardiology
- Pediatrics
- Dermatology
- Endocrinology
- Pain Management
- Gastroenterology
- Infectious Disease
- Obesity Medicine
- Rheumatology
- Nephrology
- Neurology
- Pulmonology
Hematemesis Secondary to a Bronchogenic Cyst
A 24-year-old man with an unremarkable medical history presented to the emergency department with abdominal pain and hematemesis of 3 days' duration. His symptoms were postprandial, and each episode yielded up to half a cup of blood without clots. He denied using NSAIDs or alcohol. He had had an episode of hematemesis 2 years earlier that resolved spontaneously, for which he had not sought treatment. His vital signs were normal, and his physical examination was notable only for moderate epigastric tenderness without rebound or guarding.


A 24-year-old man with an unremarkable medical history presented to the emergency department with abdominal pain and hematemesis of 3 days' duration. His symptoms were postprandial, and each episode yielded up to half a cup of blood without clots. He denied using NSAIDs or alcohol. He had had an episode of hematemesis 2 years earlier that resolved spontaneously, for which he had not sought treatment. His vital signs were normal, and his physical examination was notable only for moderate epigastric tenderness without rebound or guarding.
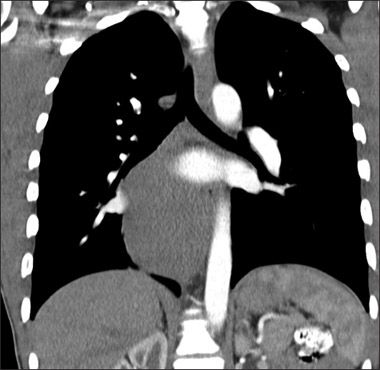
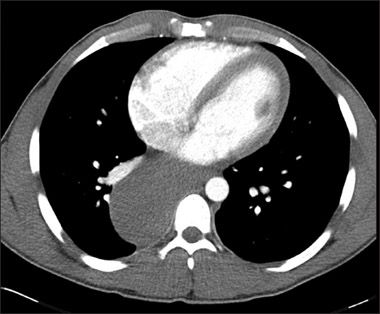
An abdominal radiographic series showed a right mediastinal soft tissue abnormality, prompting a CT scan of the chest. This showed a large 9 × 5.4 × 10-cm smoothly marginated, hypodense, homogeneous mass that emanated from the azygoesophageal recess and extended along the right aspect of the posterior mediastinum and aorta, displacing the right lower lobe of the lung and esophageal lumen. The mass was consistent with the diagnosis of a bronchogenic cyst-with esophageal duplication cyst, neuroenteric cyst, lymphangioma, and pericardial cyst included in the differential.


Bronchogenic cysts are rare congenital abnormalities that result from anomalous development of the foregut during the first trimester of gestation.1 The incidence of these abnormalities is about 20 cases per year.2 The cysts are predominantly located in the mediastinum but can also be found in the tracheobronchial tree. These thin-walled cysts are lined with respiratory epithelium and can include protein-rich mucoid material, along with varying amounts of seromucous glands, smooth muscle, and cartilage.1,3
Symptoms associated with bronchogenic cysts can include cough, hemoptysis, fever, chest pain, abdominal pain, and dyspnea. Patients may remain asymptomatic with cysts often detected incidentally during routine imaging of the chest.3 Chest radiographs usually show a dense mass; CT or MRI delineates the precise anatomical location. Because of the high rate of complications (ranging from 50% to 82% over time) and to make a specific diagnosis, surgical resection is generally recommended.1-4
References:
REFERENCES:
1.
Sarper A, Ayten A, Golbasi I, et al. Bronchogenic cyst.
Tex Heart Inst J.
2003;3:105-108.
2.
Kaur S, Goyal R, Juneja H, et al. Intrapulmonary air filled bronchogenic cyst, a rare entity.
Ind J Radiol Med
. 2006;16:865-867.
3.
Aktogu S, Yuncu G, Halilçolar H, et al. Bronchogenic cysts: clinicopathological presentation and treatment.
Eur Respir J
. 1996;9:2017-2021.
4.
Suen HC, Mathisen DJ, Grillo HC, et al. Surgical management and radiological characteristics of bronchogenic cysts.
Ann Thorac Surg
. 1993;55:476-481.








FDA Approves First Oral GLP-1 Receptor Agonist for Chronic Weight Management
December 23rd 2025The FDA approved once-daily oral semaglutide 25 mg for chronic weight management and long-term weight maintenance in adults with obesity or overweight, based on data from the OASIS clinical trial program.


Phase 3 Data Support Oral Orforglipron for Weight Maintenance After GLP-1–Based Weight Loss
December 19th 2025Topline Phase 3 ATTAIN-MAINTAIN data show oral orforglipron met primary and key secondary endpoints for weight maintenance after prior GLP-1–based injectable therapy in adults with obesity.

